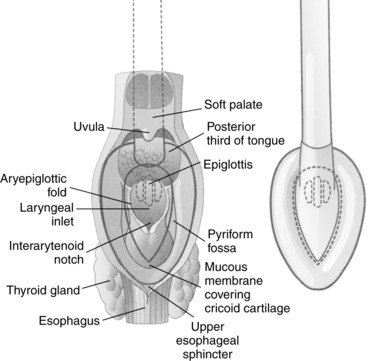
PROCEDURE 7 A laryngeal mask airway may be used to provide an emergency airway during resuscitation of a profoundly unconscious patient who needs artificial ventilation when endotracheal intubation is not readily available or has failed in establishing an airway.1 • The requirement for rapid airway management in an unconscious patient should be understood. • The anatomy and physiology of the upper airway should be understood. • The design of the laryngeal mask airway (LMA) available to the practitioner should be understood (Fig. 7-1): Figure 7-1 Components of the laryngeal mask airway. (From The Laryngeal Mask Company Limited: Instruction manual: LMA-Classic, San Diego, 2005, LMA.) • The final placement of an LMA in the airway should be understood (Fig. 7-2). Figure 7-2 Dorsal view of the laryngeal mask airway showing position in relation to pharyngeal anatomy. (From The Laryngeal Mask Company Limited: Instruction manual: LMA-Classic, San Diego, 2005, LMA.) • The ability to ventilate an unconscious patient adequately with a mouth-to-mask or bag-valve-mask device is necessary. • An understanding of the limitations of the LMA is needed. Limitations are as follows: v The presence of a nasogastric tube may make regurgitation more likely because of its effect on the esophageal sphincter tone and may also prevent the LMA from properly sealing the hypopharynx.12,13 • There are no absolute contraindications to the LMA if the alternative is loss of the airway with its associated complications.6 • The LMA may provide a more viable means of ventilation than a self-inflating manual resuscitation bag-valve-mask device in patients with a beard or without teeth.11 • Initial and ongoing training is necessary to maximize insertion success and minimize complications.8,11 • This procedure refers specifically to the LMA-Unique, a disposable model of the nondisposable LMA-Classic. Other types of LMA devices are available and provide additional features, such as endotracheal intubation through the LMA or gastric suctioning. • Two LMA-Unique devices of the appropriate size for patient weight3
![]() Laryngeal Mask Airway
Laryngeal Mask Airway
PREREQUISITE NURSING KNOWLEDGE
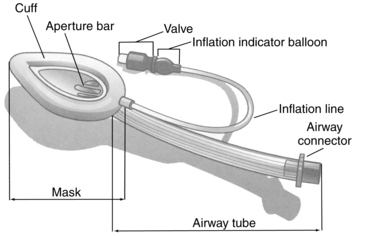
 An airway tube connects the mask and the 15-mm male adapter.
An airway tube connects the mask and the 15-mm male adapter.
 An inflation line is fitted with a valve and a pilot balloon that leads to the mask’s cuff.
An inflation line is fitted with a valve and a pilot balloon that leads to the mask’s cuff.
 The LMA does not protect the airway from aspiration of stomach contents, and the risks of insertion and aspiration must be weighed against the need to establish an airway.12
The LMA does not protect the airway from aspiration of stomach contents, and the risks of insertion and aspiration must be weighed against the need to establish an airway.12
 The LMA should not be used on patients who need high ventilator pressures (e.g., patients with pulmonary fibrosis, significant obesity) because the LMA provides a low-pressure seal.12
The LMA should not be used on patients who need high ventilator pressures (e.g., patients with pulmonary fibrosis, significant obesity) because the LMA provides a low-pressure seal.12
 The LMA should not be used in an emergency situation in which the patient is not profoundly unconscious and may resist insertion of the device.12
The LMA should not be used in an emergency situation in which the patient is not profoundly unconscious and may resist insertion of the device.12
 The LMA should be used with caution in patients with oropharyngeal trauma, only when all other means of establishing an airway fail1 and when the risks of insertion are weighed against the need to establish an airway.
The LMA should be used with caution in patients with oropharyngeal trauma, only when all other means of establishing an airway fail1 and when the risks of insertion are weighed against the need to establish an airway.
 The LMA can cause local irritation that leads to coughing and pressure lesions, which may cause 12th cranial nerve palsy.2
The LMA can cause local irritation that leads to coughing and pressure lesions, which may cause 12th cranial nerve palsy.2
EQUIPMENT
 Weight ranges listed for LMA-Unique sizes are only approximations; the size used may need to be adjusted for individual body habitus variations (i.e., patients who are short and obese may need a smaller size). Emerging clinical data suggest that use of a larger size provides an effective seal without associated higher pharyngeal pressures.3,7
Weight ranges listed for LMA-Unique sizes are only approximations; the size used may need to be adjusted for individual body habitus variations (i.e., patients who are short and obese may need a smaller size). Emerging clinical data suggest that use of a larger size provides an effective seal without associated higher pharyngeal pressures.3,7
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 14: Tracheostomy Tube Care
14: Tracheostomy Tube Care
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


7: Laryngeal Mask Airway





