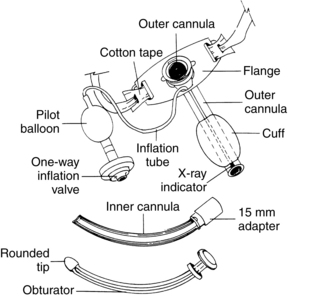
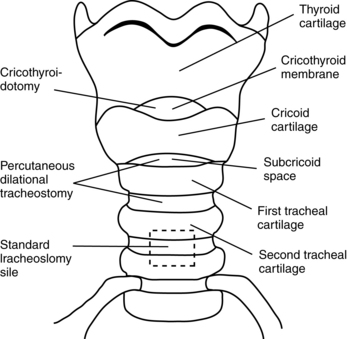
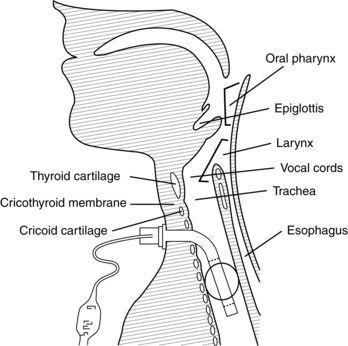
PROCEDURE 14 • Tracheotomy refers to the surgical procedure in which an incision is made below the cricoid cartilage through the second to fourth tracheal rings (Fig. 14-1). Tracheostomy refers to the opening, or stoma, made by the incision. The tracheostomy tube is the artificial airway inserted into the trachea during tracheotomy (Fig. 14-2). Figure 14-1 Sites for tracheostomy insertion. (From Serra A: Tracheostomy care, Nurs Stand 14:42,45-52, 2000.) Figure 14-2 A tracheostomy (sometimes called a tracheotomy) is created surgically by making an opening through the skin of the neck into the trachea. (Serra A: Tracheostomy care, Nurs Stand 14:42,45-52, 2000.) • Tracheostomy tubes have a variety of parts (Fig. 14-3) and are available in various sizes and styles from several manufacturers. The tubes can be metal or plastic, with standard or extra length. Clinicians who care for patients with tracheostomy tubes must understand the differences and select a tube that appropriately fits the patient and clinical condition. A tracheostomy tube is shorter than but similar in diameter to an endotracheal tube and has a squared-off distal tip for maximization of airflow. The outer cannula forms the body of a tracheostomy tube with a cuff. The neck flange, attached to the outer cannula, assists in stabilizing the tube in the trachea and provides the small holes necessary for proper securing of the tube. Some tracheostomy setups have an inner cannula inserted into the outer cannula. The inner cannula is removable for easy cleaning without airway compromise. The cuff is a balloon inflated with air to maintain a seal around the tube. As the air flows through the one-way inflation valve, the pilot balloon inflates, which indicates the volume of air present in the cuff. • A cuffed tube is appropriate for use in patients who need mechanical ventilation or for whom aspiration is a problem. The cuff limits aspiration of oral and gastric secretions. Uncuffed tubes are commonly used in children, in adults with laryngectomies, and during decannulation of the tracheostomy. A fenestrated tracheostomy tube has an opening in the curvature of the posterior wall of the outer cannula. The matching fenestrated inner cannula is inserted into the outer cannula. Fenestrated tracheostomy tubes are useful for patients with smaller tracheas and during weaning.12 With cuff deflation, options for speech are finger occlusion technique, placement of a speaking valve (Passy-Muir valve), or capping of the outer cannula; all permit air to flow through the upper airway and tracheostomy opening. Foam cuff tracheostomy tubes consist of a high-volume cuff and are composed of polyurethane foam covered with a silicone sheath. Despite the long availability of this type of tracheostomy tube, it is not commonly used and is usually reserved for patients who already have tracheal injury related to the cuff. • A tracheotomy is performed as either an elective procedure or an emergency procedure for a variety of reasons (Table 14-1). Most often, the procedure is elective and performed in the operating room with sterile conditions. An emergency tracheotomy is performed at the bedside with aseptic technique or before arrival in the critical care unit when swelling, injury, or other upper airway obstruction prevents intubation with an endotracheal tube. Percutaneous tracheotomies also are performed at the bedside. Minimally invasive percutaneous tracheotomy was introduced recently as an alternative to the traditional surgical technique. It has gained widespread acceptance in the past decade.5,8 This procedure consists of passing a needle into the trachea, placing a J-tipped guidewire, progressively dilating the trachea, and placing the tracheostomy tube. The percutaneous procedure has achieved outcomes comparable with outcomes with the surgical technique.1,3 Table 14-1 Bypass acute upper airway obstruction Prolonged need for artificial airway Prophylaxis for anticipated airway problems Reduction of anatomic dead space Prevention of pulmonary aspiration Retained tracheobronchial secretions Chronic upper airway obstruction • Protocols for emergency tracheotomy vary among institutions. Often, nurses at the bedside take an active role in assisting with tracheotomy and insertion of a tracheostomy tube; however, some institutions have surgical personnel at the bedside to assist with the procedure. • During insertion, the obturator replaces the inner cannula. Its smooth surface protrudes from the outer cannula and minimizes tracheal trauma. When the tracheostomy tube is inserted, the obturator is removed and replaced with the inner cannula, which locks in place. The same size sterile tracheostomy tube should be available at the bedside for easy access in case of accidental decannulation. • The decision for a tracheotomy in patients with long-term mechanical ventilation is made on the basis of the team’s projection regarding length of time that mechanical ventilation or an artificial airway is required. A tracheostomy tube is the preferred method of airway maintenance in a patient who needs intubation for more than 14 to 21 days. Each case must be reviewed individually.1,3,10,13,14 Better predictors are needed to further identify patients who can benefit from tracheotomy early in the course of mechanical ventilation.8
Tracheostomy Tube Care
PREREQUISITE NURSING KNOWLEDGE
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


14: Tracheostomy Tube Care