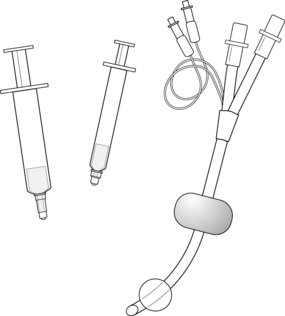
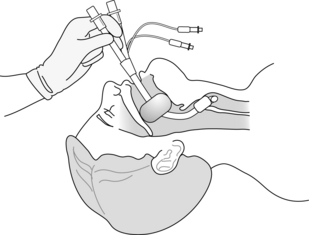
PROCEDURE 1 • Anatomy and physiology of the upper airway should be understood. • The Combitube does not require direct visualization of the airway for insertion and is inserted in a “blind” fashion, as an adjunct when endotracheal intubation attempts fail or trauma makes visualization of the airway difficult.1,8 The Combitube (Fig. 1-1) is available in two sizes, determined by patient height.12 • For patients greater than or equal to 66 inches (168 cm), the 41F size should be used. • The Combitube has a unique design that includes: • The correct placement of a Combitube in the airway is as follows: • Tracheal insertion (Fig. 1-4), in which the distal cuff occludes the trachea and the proximal balloon occludes the hypopharynx, allows ventilation through the white lumen. • Before the insertion of a Combitube, adequate ventilation of an unconscious patient with a mouth-to-mask or a bag-valve-mask device is necessary. • Use of the Combitube is contraindicated for airway management8,12 in the following cases:
![]() CombitubeCombitube Insertion and Removal
CombitubeCombitube Insertion and Removal
PREREQUISITE NURSING KNOWLEDGE
 The 37F size is used for patients 48 to 66 inches tall (122 to 168 cm).
The 37F size is used for patients 48 to 66 inches tall (122 to 168 cm).
 Either size 37F or size 41F is applicable in patients 60 to 66 inches tall (152 to 168 cm).12
Either size 37F or size 41F is applicable in patients 60 to 66 inches tall (152 to 168 cm).12
 A double-lumen, semirigid airway
A double-lumen, semirigid airway
 Blue lumen opening to the perforations between the cuffs
Blue lumen opening to the perforations between the cuffs
 White lumen opening distal to the distal cuff
White lumen opening distal to the distal cuff
 Proximal cuff (85 mL or 100 mL, depending on tube size) to occlude the hypopharynx
Proximal cuff (85 mL or 100 mL, depending on tube size) to occlude the hypopharynx
 Distal cuff (12 mL or 15 mL, depending on tube size) to occlude either the esophagus or the trachea
Distal cuff (12 mL or 15 mL, depending on tube size) to occlude either the esophagus or the trachea
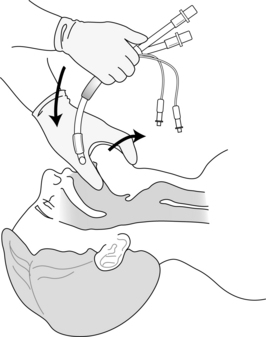
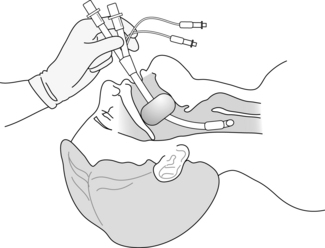
 Esophageal insertion (Figs. 1-2 and 1-3), in which the distal cuff occludes the esophagus and the proximal balloon occludes the hypopharynx, allows ventilation via the blue lumen.
Esophageal insertion (Figs. 1-2 and 1-3), in which the distal cuff occludes the esophagus and the proximal balloon occludes the hypopharynx, allows ventilation via the blue lumen.
 Patients with an intact gag reflex
Patients with an intact gag reflexRelated posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 20: Chest Tube Placement (Perform)
20: Chest Tube Placement (Perform)
![]() 95: Lumbar Puncture (Perform)
95: Lumbar Puncture (Perform)
![]() 35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


1: Combitube Insertion and Removal