CMRO2. However, severe brain injury may lead to disruption of the autoregulation of CBF such that too much or too little CBF may be supplied for the metabolic demands of the brain.
Table 9.1 Central Nervous System Alterations in Surgical Critical Illness | |
|---|---|
|
 Figure 9.1 A schematic representation of the reticular activating system arising from the brainstem and projecting impulses cephalad throughout the cortex. Source: ACS. ATLS Student Manual. Chicago: ACS, 1997. |
low, indicating increased oxygen extraction. Continuous measurement of jugular oxygen saturation (SjvO2) has been used as a monitor of global cereberal oxygen delivery and consumption, especially in patients with TBI. Normal jugular venous oxygen saturation is 55-71%. Values <50% are usually secondary to decreased delivery rather than increased consumption (2, 3, 4).
 Figure 9.2 The interior of the base of the skull illustrating the bony prominences, which can result in direct or counter-coup injury to the brain. Source: Romanes CJ. Cunningham’s Manual of Practical Anatomy. New York, NY: Oxford University Press, 1978. |
 Figure 9.3 An open skull depicting the tentorium and the position of midbrain in juxtaposition to the medial, anterior tentorium, and adjacent to the location of the temporal lobe. Source: ACS. ATLS Student Manual. Chicago: ACS, 1997. |
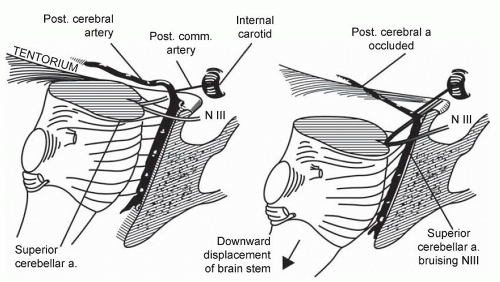 Figure 9.4 A schematic representation further depicting the close application of the tentorium and, therefore, the temporal lobe to the midbrain, the oculomotor nerve and the brainstem circulation. Source: ACS. ATLS Student Manual. Chicago: ACS, 1997. |
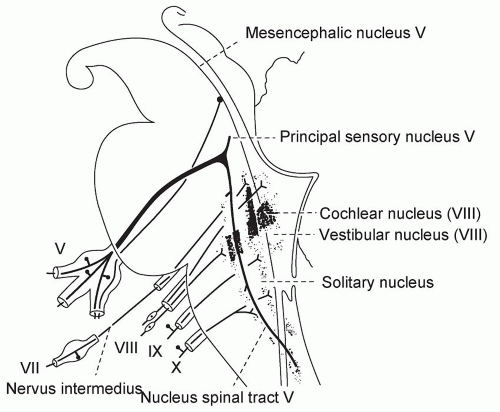 Figure 9.5 A schematic representation of the sensory nerves of the brainstem with the midbrain devoid of major sensory nerves, the pons with the fifth nerve, important for the corneal reflex, and the eighth nerve at the pontomedullary junction, important for the oculocaloric reflexes. Source: Gray’s Anatomy, 28th edn. Baltimore: Lea & Febinger, 1968. |
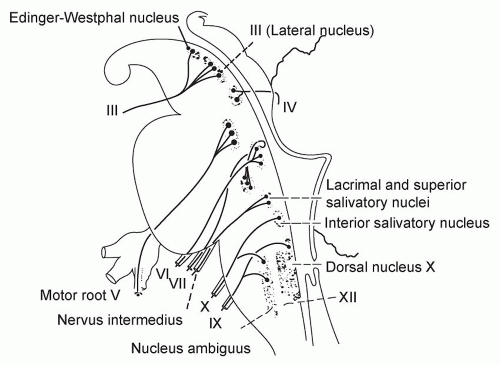 Figure 9.6 A schematic representation of the motor nerves of the brainstem, with the midbrain contributing the Edinger-Westphal nucleus for parasympathetic innervation of the pupil, and the third nerve that is important for oculovestibular and oculocaloric reflexes. The pons contributes the sixth nerve, also important for oculovestibular and oculocaloric reflexes, as well as the seventh nerve that is important for the corneal reflex. Source: Gray’s Anatomy, 28th edn. Baltimore: Lea & Febinger, 1968. |
Table 9.2 Determinants of Increased Intracranial Pressure | |
|---|---|
|
The exact duration of absent circulation that will cause irreversible cortical and subsequent brainstem death is controversial.
Table 9.3 Glasgow Coma Scale | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
CMRO2 (normal 3.2) | GCS (normal 15) |
1.1 | 3-4 |
1.5 | 5-6 |
1.5 | 7-8 |
Table 9.4 Etiologies of Coma | |
|---|---|
|
in trauma patients, and may indicate increased ICP or injury to the sympathetic nervous system in the high spinal cord. Similarly, hypertension is less common than hypotension, and can result from increased ICP. Since many critically ill surgical patients are assisted by a ventilator, respiratory status is a less useful indicator of neurological function, except for the broad categories of present or absent.
Table 9.5 Outline of Physical Examination for Brain Status | |
|---|---|
|
ABC of trauma and continuing attention to oxygenation and resuscitation of the circulation are as, if not more, important with brain injury as with any other injured tissues. Previous ideas that brain injury could be limited by providing minimal resuscitation of the circulation are not supported by epidemiologic studies that demonstrate an increased risk of death and neurologic disability in brain-injured patients who suffer from hypotension anytime during the early post-injury period (13, 14, 15, 16).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


