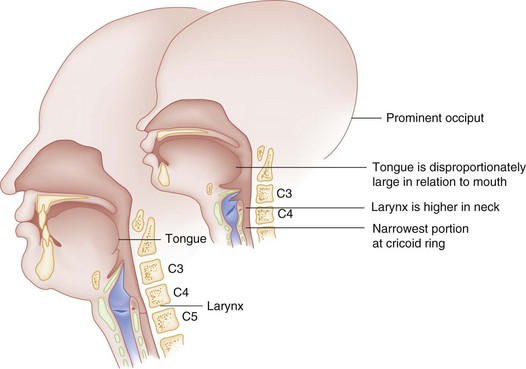
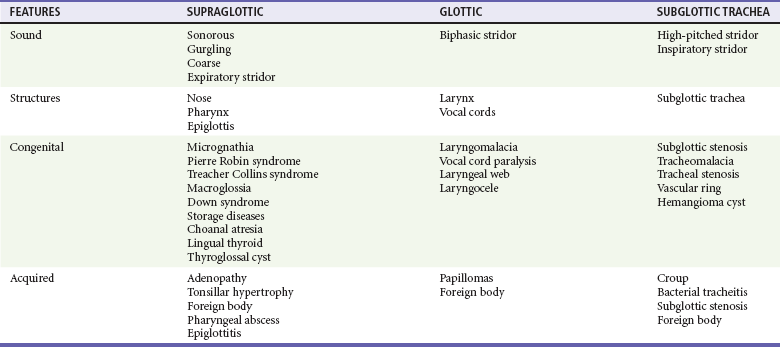
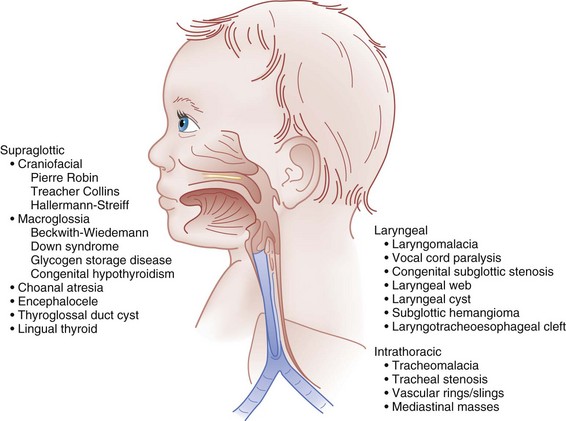
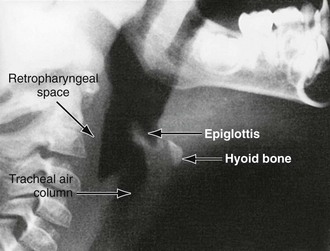
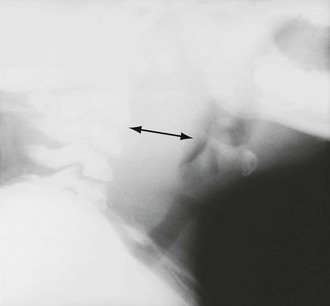
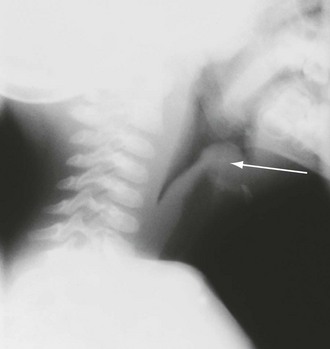
Chapter 168 A number of differences between the adult and pediatric airway are important in airway management (Fig. 168-1). An infant’s tongue is disproportionately large in relation to the mouth and protrudes back into the posterior of the pharynx. In the setting of hypotonia, posterior displacement of the tongue is the most common cause of functional upper airway obstruction. The infant larynx is more anterior and higher in the neck relative to the cervical spine (at C3-4) compared with an adult larynx (C4-5). The anterior aspect of the vocal cords is tipped inferiorly. The narrowest site of the infant airway is at the cricoid ring rather than the cords as in an adult. A child’s epiglottis is relatively larger, longer, and omega shaped. It extends vertically beyond the opening of the cords, thus making a complete view of the airway difficult. The caliber of all airway structures is small; on average, newborn tracheal length is 57 mm and laryngeal diameter is 4 mm. All cartilaginous supporting structures are soft, pliable, and prone to collapse. Finally, a prominent occiput causes passive flexion of the head and neck on the cervical spine. In aggregate, these anatomic features of the pediatric airway predispose infants and young children to functional upper airway obstruction and make airway intervention technically challenging. The type and size of equipment required for management of the pediatric airway are derived from this unique anatomy. A face mask should be sized so that the top and bottom rims fit on the bridge of the nose (below the eye) and in the cleft of the chin. A straight (Miller) blade is generally used for endotracheal intubation in infants and young children because the tip of the straight blade lifts the epiglottis up and out of the line of vision of the airway. Endotracheal tube size is a function of the patient’s size. For children older than 1 year, endotracheal tube size (internal diameter in millimeters) can be estimated by the formula (age in years/4) + 4; for uncuffed tubes, a half size smaller than calculated should be used, except for 3.0-mm tubes. Alternatively, endotracheal tube size can also be estimated by use of a length-based measuring system, such as the Broselow-Luten tape. Recent evidence suggests that cuffed endotracheal tubes may be used safely in children of all ages. Cuffed endotracheal tubes allow the delivery of high pressures during ventilation without the air leak associated with uncuffed tubes and without increased complications, such as subglottic stenosis.1 • Acute infections of the upper airway range from relatively mild distress and self-limited signs and symptoms to the abrupt onset of a rapidly progressive airway obstruction. • Undiagnosed congenital anomalies of the airway and surrounding structures may be manifested as chronic or progressive stridor or simply difficulty in feeding. An infant with a congenital airway anomaly in whom an acute airway infection develops is at higher risk for decompensation and respiratory failure. • Upper airway obstruction from a foreign body in the airway or esophagus can cause partial or complete airway obstruction and may require urgent advanced airway management skills. Stridor is the classic sound associated with upper airway obstruction.2–4 It is derived from the Latin stridulus, meaning harsh or grating. Stridor is caused by partial airway obstruction and the resultant turbulent airflow through some portion of the airway from the nose to the trachea. It is not a diagnosis in itself but an important sign that must be investigated in the symptomatic patient. Stridor should be described in its timing within the respiratory cycle (inspiratory, expiratory, biphasic) and by its quality (coarse or high pitched) (Table 168-1). The upper airway can be artificially divided into four regions: the nose and pharynx, the supraglottic structures, the glottis and immediate subglottic area, and the intrathoracic trachea (Fig. 168-2). The characteristics of stridor differ by its cause and its precise origin in the airway. • Onset and duration (acute vs. chronic) • Associated symptoms (respiratory distress, fever, toxicity, drooling, cyanosis) • Progression with age (number of bouts and severity of “croup” with increasing age) • Exacerbating factors (supine vs. prone position, upper respiratory infection [URI], crying) • Feeding pattern (dysphagia, feeding abnormalities) • Prior airway procedures (intubation in the neonatal period) • Choking episode (foreign body aspiration) • Baseline noises, quality of cry and voice (to help in location of obstructive lesion) Radiographs of the soft tissues of the neck may be helpful and should include both lateral and anteroposterior views. These views assess the adenoid and tonsillar size, the contour of the epiglottis, the thickness of the retropharyngeal soft tissue space, the vallecula, the aryepiglottic folds, and the tracheal air column (Fig. 168-3).5,6 Optimally, the child’s head should be positioned in extension and the film taken during inspiration. Views of the chest may be helpful to assess the heart size, the trachea and bronchi, the location of the aortic arch, and the presence of other pulmonary pathologic processes. Perspective.: A retropharyngeal abscess is a potentially life-threatening airway emergency resulting from infection of the retropharyngeal soft tissue space. The retropharyngeal space is a potential space between the posterior pharyngeal wall and the prevertebral fascia that extends from the base of the skull to the level of T2. It is rich in lymph tissue that drains the nose, pharynx, sinuses, and ears. An abscess may result from direct trauma from a fall with an object in the mouth like a toothbrush, suppuration of lymph nodes, contiguous spread of infection, or hematogenous seeding.7 Approximately 50% of pediatric cases occur in children 6 to 12 months of age. Almost all of the pediatric cases occur before 3 years of age, and 96% of all diagnosed pediatric retropharyngeal abscesses are seen before 6 years of age.8 These infections are commonly polymicrobial, with Streptococcus and anaerobes the most commonly isolated organisms.9 Recent case reports highlight the emerging role of methicillin-resistant Staphylococcus aureus in these infections.10 Clinical Features.: The variable presentation of a retropharyngeal abscess can make it a challenging diagnosis in young children.11–14 Common signs and symptoms include fever, sore throat, neck stiffness or nuchal rigidity, torticollis, trismus, neck swelling, drooling, stridor, and muffled voice. In a prospective study of 17 patients with retropharyngeal abscess, stridor and airway obstruction were observed in approximately half (56%) of the patients.15 This common finding of acute airway obstruction is a function of the high position of the larynx in the neck. Such anatomy places the airway proximate to and easily compressed by the bulging retropharyngeal mass. In patients with airway compression, the clinical appearance can resemble epiglottitis. Reluctance to extend the neck and an unwillingness to look side to side is often seen with retropharyngeal abscess and may help differentiate it from other supraglottic infections.16 With less obvious signs of airway obstruction, patients can exhibit a mixture of symptoms (fever, neck stiffness, generalized toxicity) that may also suggest meningitis or sepsis. Other serious complications of retropharyngeal abscess include aspiration pneumonia, mediastinitis, and empyema. Diagnostic Strategies.: Careful evaluation of airway patency takes precedence in management of a child with a presumed retropharyngeal abscess. Examination of the pharynx may reveal bulging of the posterior pharyngeal wall. A soft tissue lateral view of the neck may be helpful to establish the diagnosis; in the normal patient, the width of the retropharyngeal space should not exceed the diameter of the adjacent vertebral body (Fig. 168-4). In general, soft tissue width should not be larger than 7 mm at C2 or exceed 14 mm at C6. The majority of patients (in some studies 88-100%) will demonstrate retropharyngeal thickening on the lateral neck radiograph.8,17,18 An air-fluid level is more commonly seen with perforations and anaerobic infections. Redundant soft tissue of the retropharyngeal space complicates interpretation of lateral neck films in young infants with a retropharyngeal abscess. Artifactual widening of a normal retropharyngeal space is commonly seen when the radiograph is taken with the head and neck in flexion or during exhalation (or both). CT may be beneficial in delineating the size and extent of an abscess and determining possible impingement on airway structures. Before the patient is placed in the CT scanner, the ability to tolerate being supine should be tested, and staff and airway equipment should be immediately available. Management.: The size of the abscess, the degree of airway obstruction, and the overall toxicity of the patient dictate management. The need for intubation or surgical drainage is determined on an individual basis, and these patients generally benefit from involvement of an ear, nose, and throat (ENT) specialist. Intubation can be complicated by distorted anatomy and can lead to abscess rupture.19 Not all retropharyngeal abscesses require surgical drainage as many will respond to intravenous antibiotics. A study by Craig and Schunk showed a resolution rate with antibiotics of 37%.20 Clindamycin is a common appropriate first choice for antibiotic therapy. Peritonsillar Abscess.: Peritonsillar abscess more commonly occurs in older children and teenagers. Although it can cause drooling and a muffled, hot potato voice, severe respiratory distress is less common. Peritonsillar abscess is associated with trismus, bulging or asymmetry of the tonsils, and deviation of the uvula away from the abscess side. Throat pain also may radiate to the ear.7 Treatment involves antibiotics and either incision and drainage or, more commonly, needle aspiration. Posterior pharynx ultrasonography or CT scanning can confirm the diagnosis and help guide treatment. Any drainage effort must take great care to avoid puncture of the proximate carotid artery or aspiration of drained material by the patient. Mononucleosis.: Infectious mononucleosis, caused by the Epstein-Barr virus, can lead to mucosal edema and an exudative pharyngitis. Uncommonly, massive tonsillar enlargement can occur and create upper airway distress. In addition to airway management and general supportive care, some studies have shown benefit of steroids and racemic epinephrine in reducing tonsillar edema.21,22 Ludwig’s Angina.: Ludwig’s angina is a rapidly progressive infection and inflammatory process of the sublingual, submandibular, and submaxillary spaces. Elevation of the tongue above the lower teeth and tenderness in the sublingual space are hallmark signs along with trismus and odynophagia. It can create a functional upper airway obstruction or respiratory distress through significant swelling and direct airway compression. CT is useful to confirm the diagnosis and extent of infection; treatment involves antibiotics, airway support, and admission for close monitoring. ENT and anesthesia consultants can help in planning and support if an emergent airway is required. Perspective.: Although it is still a feared pediatric emergency, acute epiglottitis has declined markedly in incidence since widespread administration of Haemophilus influenzae type b vaccine.23–25 First licensed in 1985 for children 24 months old, the vaccine became available for immunization of infants 2 months of age in 1990. Principles of Disease.: Epiglottitis is an invasive bacterial disease that causes inflammation and edema of the epiglottis, aryepiglottic folds, arytenoids, and surrounding supraglottic tissues. As these structures become inflamed and distended, they protrude downward and over the glottic opening. Uncommon in the first year of life, epiglottitis was historically caused by H. influenzae type b in children 3 to 7 years of age and occurred year-round. This traditional profile has changed.26–28 In a survey of patients with epiglottitis since 1990, the average patient is older (80 vs. 35 months) with varying microbiology. H. influenzae type b is seen in a small minority of patients, and organisms such as group A beta-hemolytic streptococcus, S. aureus, and Streptococcus pneumoniae are more common.29 Noninfectious causes are rare and include thermal injury from swallowing of hot liquids.30,31 Clinical Features.: Epiglottitis is classically acute in onset. It is marked by high fever, intense sore throat, toxicity, and rapid progression. In one study, 85% of children with epiglottitis were symptomatic for less than 24 hours before seeking medical care.32 Children with epiglottitis appear anxious and maintain a “sniffing” or “tripod” position with the jaw jutting forward and the neck extended to maximize airway patency. As symptoms worsen, cough and phonation are usually absent. Drooling is prominent because of an inability to swallow.33 Singer and McCabe showed that in children younger than 24 months, toxicity, altered mental status, dyspnea, stridor, retractions, and fever are common initial symptoms.34 Losek and co-workers reported a series of 236 patients in which 7 patients (3%) died. In addition, the correct diagnosis of epiglottitis was not made in 11 of 58 children younger than 2 years (19%) and in 49 of 178 children between 2 and 18 years old (28%). Incorrect diagnoses in patients who died of epiglottitis included croup, summer virus, and pharyngitis. Croup was the most commonly assigned misdiagnosis and more often made in the setting of very young children or those in whom drooling and difficulty in swallowing were not prominent.32 The older patient is less likely to show dramatic signs of upper airway obstruction compared with the younger child because the diameter of the airway is larger and thus takes a greater degree of swelling to produce symptoms. Epiglottitis caused by bacteria other than H. influenzae tends to have a slower onset and is less likely to cause airway compromise. A majority of patients with H. influenzae epiglottitis were also found to have bacteremia (50-75%).35 Diagnostic Strategies.: Direct examination or manipulation of the pharynx should be avoided in cases in which epiglottitis is strongly suspected. A lateral neck radiograph can be helpful to confirm the diagnosis and should be evaluated for an enlarged epiglottis (“thumbprint sign”; Fig. 168-5), thickened aryepiglottic folds, lack of air in the vallecula, and dilated hypopharynx. Careful observation of a child with suspected epiglottitis is essential, and clinicians skilled in airway management should accompany the patient at all times. Laboratory tests, intravenous fluids and antibiotics, and blood and epiglottis cultures are all important considerations once the airway has been secured. Figure 168-5 Epiglottitis. Note the “thumbprint sign” of the epiglottis and thickened aryepiglottic folds.
Pediatric Respiratory Emergencies
Upper Airway Obstruction and Infections
Distinguishing Principles of Disease
Stridor
Overview of the Evaluation and Management of a Child with an Upper Airway Obstruction
Specific Disorders
Infectious Etiologies
Epiglottitis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree