Chapter 5 Classification of muscles
General overview
Hannon1 describes muscles as having a wide variety of functions serving as springs, engines, braces and brakes. Attempting to understand these versatile roles, scientists and clinicians have variously classified muscles according to certain characteristics such as morphology, actions or functional role. These are explored.
Individual muscle morphology
Morphology refers to the basic form or structure of a muscle. This involves two aspects:
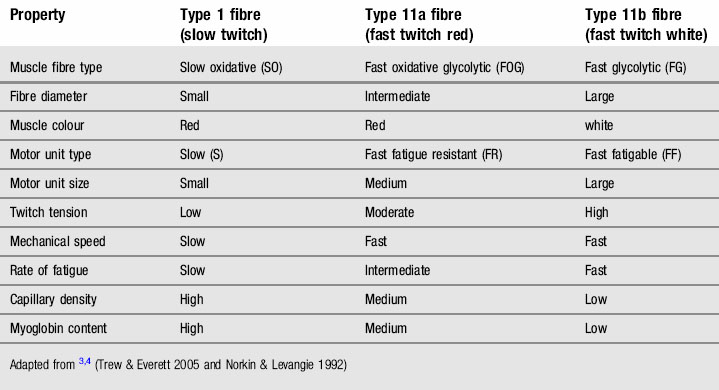
According to Trew and Everett,3 during low force contractions of a muscle, only Type 1 fibres may be recruited and so these are used mainly for normal everyday activities which do not require maximal or high force contractions. Their resistance to fatigue suits them well for this role. As the force generated by the muscle increases, the Type 11 fibres are progressively recruited and during maximal activity all motor units are involved. However maximal force rapidly declines due to the high fatigue rate of the force generating fibres. There is a wide variation in the proportion of the different fibre types between muscles and between people. Each person has a unique proportion of Type 1 to 11 fibres and the fibre type is largely determined genetically.3 Each motor unit within a muscle contains fibres of only one type.5
Limb immobilization studies have demonstrated a conversion of fibre types with a decrease in slow twitch fibres and increase in the proportion of fast twitch.6
Classification of muscles according to functional role
In attempting to simplify and aid the conceptual understanding of the complex roles that muscles perform, various different functional classification systems have been adopted. However, the different nomenclature used has to some extent confused the issue and there is a lack of general consensus on the subject. Each aspect is examined and a more holistic and inclusive classification system is subsequently proffered.
Tonic and phasic muscles
Tonic muscles are those with a predominance of Type 1 fibres. These muscles work at a low grade of contraction in a sustained manner thus have a lot of endurance. They are often also termed stability or postural muscles as they help to maintain stability of the body,4 e.g. the soleus is almost continually active in standing and owing to the high proportion of Type 1 fibres can make small adjustments in muscle tension required to maintain body balance and counteract gravity.
Phasic muscles are those muscles with a predominance of Type 11 fibres. These play a major role in large movements and those requiring more power and speed. They are either called mobility or phasic muscles. However, they fatigue more quickly and following intermittent bouts of high intensity exercise recover more slowly than the tonic muscles,4 e.g. the gastrocnemius. Table 5.2 presents the more commonly used distinguishing features4 of the tonic and phasic muscles.
Table 5.2 Different characteristics of tonic and phasic muscles (after Norkin and Levangie4)
| Tonic | Phasic | |
|---|---|---|
| Fibre type | High proportion Type 1 fibres | High proportion Type 11 fibres |
| Fibre arrangement | Penniform | Parallel |
| Location | Deep and cross one joint | Superficial and cross more than one joint |
| Primary function | Stability | Mobility |
| Action | Extension, abduction and external rotation | Flexion adduction and internal rotation |
Besides the differences in function and structure outlined above, Kolar7 importantly draws attention to the differences in the neural control of the different muscle fibres – it is the type of the motor neuron which determines the type of muscle fibre, creating either tonic or phasic motor units. This difference becomes particularly striking in the light of our individual motor and phylogenetic or evolutionary development. At birth, the infant’s posture is predominantly influenced by the phylogenetically older phasic (as described in Table 5.2) muscle system. (Kolar calls this the tonic system!) The tonic system (Table 5.2) is less evident, but as the central nervous system (CNS) matures these muscles play an increasingly important part in the development of upright posture and its stabilization with movement (Kolar calls this system the phasic system). This system is phylogenetically younger, more vulnerable and tends to become weak. Maturity of this system is not achieved until the child is 4 years old.
It is important to point out at this point that the nomenclature used by the Czech School of Manual Medicine can be confusing and appear contradictory as is evidenced by the paragraph above. This may account for a less wide understanding and acceptance of their valuable work. In addition it may contribute some of the current confusion on the subject. Their use of the terms tonic and phasic is different to that shown in Table 5.2, and further compounded when talking of postural and phasic muscles. This is further elaborated upon when examining Janda’s classification, and the muscle classification debate (see p. 60).
Kolar7 does clarify that tonic motor units have a more postural role and phasic motor units have a more kinetic role and that both motor units are present in differing proportions in every muscle. However, he also adopts the nomenclature used by Janda making his work more difficult to interpret.
Importantly, Kolar7 questions which position is decisive in opposing gravity and I agree. He sees that in motor control, both types of muscles have dual functions participating in both posture and movement. The decisive difference between them consists of the timing of their development. Postural activity of the tonic system (his phasic) comes into play as central nervous control becomes more highly developed. The functioning between the two systems needs to become integrated and balanced.
Muscle classification according to Vladimir Janda
Professor Janda saw that the muscular system lies at a functional crossroad because it is influenced by stimuli from both the central nervous system and musculoskeletal system.8 From the clinical point of view, Janda’s significant contribution has been to show that dysfunction in the muscular system is usually a reflection of dysfunction in the peripheral or central neural system. Impaired central motor regulation results in defective or uneconomical movement patterns. As a consequence, imbalanced action between two structurally and functionally different muscle groups occurs in a systematic, regular and predictable manner.9 He proposed a more general classification of muscles throughout the body into two groups based on characteristics of their structure and function and observed actions in the clinical situation. They are the ‘postural muscles’ which are prone to over-activity which in turn tends to create relative underactivity in the antagonistic ‘phasic muscles’. These functional differences are further elaborated:
The ‘phasic muscles’ are prone to inhibition, hypotonia, atrophy and weakening and are less readily activated in most movement patterns, particularly under conditions of injury fatigue and stress. He classified certain muscles into either functional group as shown in Table 5.3.
Table 5.3 Functional division of muscles according to Janda8,10
| Postural: tightness prone muscles | Phasic: weakness prone muscles |
|---|---|
Janda defined the muscles which tend to become short and tight as those having an antigravity postural function, particularly those activated when standing on one leg. Janda5 considered the postural muscles were approximately one-third stronger than those prone to inhibition. In subjects with altered or poor movement patterns their degree of activation increases. In addition, he notes that in certain structural lesions of the CNS, as seen in cases of cerebral vascular accident or cerebral palsy, the muscles which show evident spasticity are the same as those included in the postural group.
Janda himself said there were a lot of misconceptions and discrepancies about the use of the term ‘postural muscles’.11 However, examining his muscle system groupings it is apparent that they more closely resemble the phasic muscles as described in Table 5.2.
His nomenclature is confusing for our purposes as you will see (p. 60). However, conceptually and functionally his approach has been very helpful.
Local and global muscles acting on the lumbar spine
Bergmark12 in examining the conditions for mechanical stability in the lumbar spine presented a concept of functional muscle classification into local and global muscles as they acted to control local stability in the lumbar spine including transfer of load between the thorax and pelvis (Fig. 5.1)
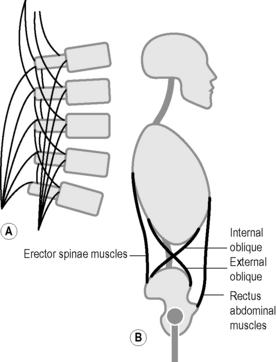
The local system includes ‘all those muscles which have their origin or insertion (or both) at the lumbar vertebrae with the exception of psoas’. The muscles included are shown in Table 5.4. This system is involved in the posture of the lumbar spine and used to ‘control the (lumbar) curvature and to give sagittal and lateral stiffness to maintain mechanical stability of the lumbar spine’.
Table 5.4 Local and global muscles of the lumbar spine described by Bergmark12
| Local muscles | Global muscles |
|---|---|
 of the muscle area
of the muscle areaThe global system ‘consists of the active components i.e. the muscles and IAP which transfer the load directly between the thoracic cage and pelvis’. The muscles have ‘origin on the pelvis and insertions on the thoracic cage’. These include the global muscles shown in Table 5.4. The main role of this system ‘appears to be to balance the outer load so that the resulting force transferred to the lumbar spine can be handled by the local system. Thus large variations of the distribution of the outer load should give rise to only small variations of the resulting load on the lumbar spine. The local system therefore is essentially dependent upon the magnitude (not the distribution) of the outer load and of the posture (curvature) of the lumbar spine’.
The influence of Bergmark:stabilizers and mobilizers
Richardson et al14., collectively known as The Queensland Group, have produced some fine research and have been at the forefront of the motor control approach to effective lumbopelvic stabilization in the treatment of low back pain. They have been strongly influenced by Bergmark as seen in Table 5.5, choosing to include transversus abdominus and some of internal oblique into the local group.14,42
Table 5.5 Categorization of the lumbar and abdominal muscles based on their role in stabilisation according to Richardson et al.14
| Local stabilizing system | Global stabilizing system |
|---|---|
In addition, Richardson13 also makes distinction between monoarticular, bi-articular and multijoint muscles. Their capacity to provide joint stabilization differs in each category. The monoarticular muscles could also be called local muscles. The multijoint muscles are phylogenetically the oldest and can be called the global muscles.13
Comerford and Mottram15 have interlinked the concepts of local/global and stabilizer/mobilizer into what they see as a more clinically useful classification. This encompasses three different functional muscle roles: local stability muscles; global stability muscles; global mobility muscles. Some muscles stabilize and some mobilize.
However, there are inherent problems for understanding functional control in seeing some muscles as stabilizers and others as mobilizers. As we have seen in Chapter 3 in the process of motor development, movement and stability develop together and are always in constant interaction in mature motor behavior. Kolar7 points out that any muscle may be required to work in a stabilizing role one moment and then as a movement producer the next. While some muscles may appear to have a predominantly stabilizing role e.g. the local muscles in the lumbar spine as described by Bergmark, importantly, they also sub serve a postural role and are also producers of fine subtle movements as well as being controllers and discrete adjusters. Danneels et al.16 found increased multifidus action in concentric lifting which could indicate that it participates in torque production. It is an oversimplification of function and erroneous to consider that they do not produce any appreciable movement and ‘just stabilize’.
Cholewicki and VanVliet17 refute the classification of muscles into local and global as a means for discriminating between muscles responsible for intersegmental stability and spine motion. All trunk muscles contribute to spine stability and their contribution depends upon many variables including posture and loading conditions. McGill18 and Kavcic et al.19 express similar sentiments. The patterns of muscle activation change as the form and magnitude of spine loading patterns change (See ‘spinal stability’ p. 86).
Muscle classification debate
In 2000, the Journal of Bodywork and Movement Therapies published a paper entitled ‘The muscle designation debate: the experts respond’.20 The paper was a response to readers who had communicated their confusion over the apparent contradictions in the way that different researchers and clinicians refer to muscle categorizations. The editor says ‘When words postural/phasic or stabilizer/mobilizer are applied to particular muscles practical as well as linguistic difficulties become apparent’.20 The preceding classification summary highlights the problem.
The principal confusion probably stems from Janda’s use of the terms postural and phasic muscles (see page 57). Comparing Table 5.2 – tonic and phasic muscles with Table 5.4 – postural and phasic muscles of Janda – we see that frequently his ‘postural muscles’ equate more to the muscles with a high Type 11 fibre content which are actually phasic muscles as defined in Table 5.2. Janda later tended to describe the postural muscles more in terms of ‘tightness prone’ while still maintaining that they were the ones predominantly activated when standing on one leg – the primary posture, according to him. The confusion becomes further compounded when both he8 and Kolar7 at times use the term ‘tonic muscle system’ referring to those muscles as described in his ‘postural group’ when in fact they are describing phasic muscle activity. Kolar7 however, does also allow that tonic motor units have a postural role.
Most of the respondents in the above mentioned paper appeared to be in agreement that phasic muscles (as defined in Table 5.2) equate to global muscles, mobilizer muscles, kinetic muscles, and, by inference, Janda’s postural muscles. Muscles with a more postural function have a greater proportion of Type 1 fibres and tonic motor units and have tended to be called local or stabilizer muscles. They behave with some similarity to Janda’s phasic muscles as he described them.









