INTRODUCTION AND EPIDEMIOLOGY
The wrist is the area from the distal radius and ulna to the carpometacarpal joints. It is a complex unit with articulations among the eight carpal bones and the distal radius and ulna. Wrist injuries are common, accounting for 2.5% of ED visits annually.1 Clinical diagnosis is often difficult, and even subtle injuries may lead to significant impairment if not properly diagnosed and treated. Management options vary from conservative to surgical, so an understanding of the functional anatomy, mechanisms of injury, and clinical evaluation is needed for proper diagnosis and treatment.
ANATOMY
The distal radius is the only forearm bone that articulates directly with the carpal bones (scaphoid and lunate). The distal radius has three articular surfaces: radiocarpal, distal radioulnar, and the triangular fibrocartilage complex. The radiocarpal surface is concave and tilted in two planes. It has an ulnar inclination, or tilt, of 15 to 25 degrees in the frontal plane, and a volar tilt of 10 to 15 degrees in the sagittal plane2 (Figure 269-1). The ulna is separated from the carpal bones by the triangular fibrocartilage complex, the main stabilizer of the distal radioulnar joint, on its distal end. The triangular fibrocartilage complex forms a smooth, continuous, ulnarly directed extension of the distal radial surface, and supports the lunate and triquetrum on the distal ulna. The distal radius has a concave sigmoid notch at its ulnar aspect that articulates with the curvature of the ulnar head, which permits wrist rotation during pronation/supination of the forearm.3 The distal radioulnar joint is also supported by dorsal and volar radioulnar ligaments that merge with the triangular fibrocartilage complex.4
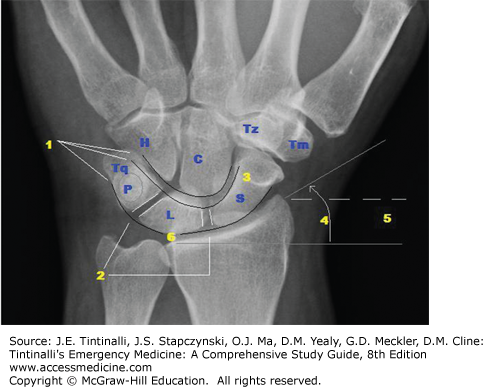
FIGURE 269-1.
Wrist. Normal posteroanterior (PA) view. 1. The carpal bones are arranged in two rows forming three smooth arcs (Gilula lines). 2. The carpal bones are separated by a uniform 1- to 2-mm space. 3. The scaphoid (S) is elongated. 4. The radius has an ulnar inclination of 13 to 30 degrees. 5. The radial styloid projects 8 to 18 mm. 6. Half the lunate articulates with the radius, with equal length over the ulna (neutral ulnar variance). C = capitate; H = hamate; L = lunate; P = pisiform; Tm = trapezium; Tq = triquetrum; Tz = trapezoid.
Eight carpal bones are arranged in two rows. The distal carpal row (trapezium, trapezoid, capitate, and hamate) is joined tightly together and to the adjoining metacarpals. The distal row is quite sTable and moves with the metacarpals as a unit in a relatively sTable arch. The proximal carpal row (scaphoid, lunate, triquetrum, and pisiform) is also arranged in an arch between the distal radius and the distal carpal row. In this arrangement, the proximal row functions as a mobile link, or “intercalated segment,” and is potentially unsTable by virtue of this position. The scaphoid is critical to wrist stability, by acting as a stabilizing strut and linking the proximal and distal carpal rows at the radial aspect of the wrist. This position explains the scaphoid’s greater propensity for injury.
Forearm muscles that insert onto the bases of the metacarpals produce wrist motion. Except for the pisiform, a sesamoid bone of the flexor carpi ulnaris, there are no direct tendon insertions on the carpal bones.5 The carpal bones move passively in response to hand position. Often, the radiocarpal joint is referred to as the “wrist joint.” However, wrist motion is divided almost equally between the radiocarpal and midcarpal joints.6 This is best understood by viewing carpal movement from the sagittal view. During flexion and extension of the wrist, each row moves in the same direction with similar degrees of angulation.
The carpal bones are stabilized to one another by intrinsic ligaments and to the bones of the forearm by extrinsic ligaments. The key extrinsic ligaments are arranged in three arcades, two of which are volar and one dorsal. The two volar ligaments are arranged in two inverted V-shaped arches, and are thought to play a major role in stabilizing the wrist. The apex of one arch inserts on the lunate supporting the proximal carpal row, whereas the other arch reaches to the distal carpal row, inserting on the capitate. The area between these two palmar arches is inherently weak and is known as the space of Poirier (Figure 269-2). This space lies at the junction of the capitate and lunate and widens upon dorsiflexion of the wrist. Forceful dorsiflexion may tear the capsule here and produce a lunate or perilunate dislocation. The single dorsal arcade has its origins on the rim and styloid of the radius on one side and distal ulna/triangular fibrocartilage complex on the other. This ligament is less important for wrist stability, acting as a sling across the dorsum of the wrist.6
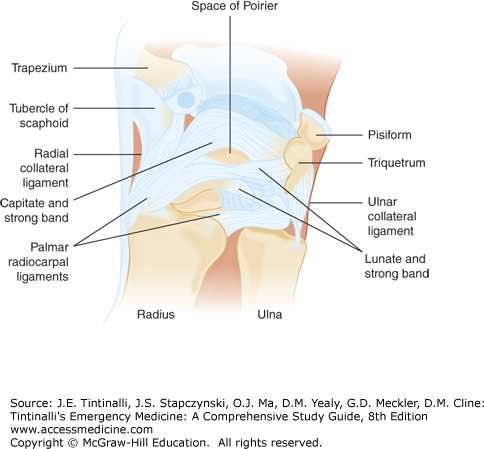
The space of Poirier is on the volar aspect of the wrist and is inherently weak. It is the site of disruption in perilunate and lunate dislocations. The intrinsic ligaments are largely responsible for holding the carpal bones together as a kinematic unit in their respective carpal rows. The intrinsic ligaments of the mobile proximal carpal row are particularly important because of their greater propensity for injury. The intrinsic ligaments of the proximal carpal row are named after the respective carpal bones they connect: the scapholunate and triquetrolunate. The palmar flexed posture of the scaphoid produces a flexion torque on the lunate that is counterbalanced by an extension torque from the triquetrum. This delicate balance is lost if either ligament is disrupted, producing a dorsal or volar tilt of the proximal carpal row and carpal instability.
PATHOPHYSIOLOGY
It is helpful to understand the mechanism of injury when assessing wrist injuries. Most injuries are caused by a fall creating an axial load on an outstretched arm and dorsiflexed wrist and hand. Impact on the thenar eminence is likely to injure the scaphoid and its supporting ligaments. An impact on the hypothenar eminence is likely to cause injury to the triquetrum, pisiform, and their supporting ligaments. Age affects the maturity of the bones and predisposes patients to certain types of injury.7 Children are likely to sustain injuries to the immature, weaker epiphyseal plate or metaphysis of the radius, sparing the still-cartilaginous carpal bones.8 Young adults, particularly those with active lifestyles, are likely to be injured with greater force and disrupt either the scaphoid, proximal row intrinsic ligaments, or distal radial metaphysis.8 In the elderly, especially with underlying osteoporosis, the weak point is the brittle distal radial metaphysis, resulting in a Colles fracture, often with intra-articular involvement.9
CLINICAL FEATURES
Begin assessment by looking at both wrists to assess for symmetry and range of motion in dorsiflexion, palmar flexion, and radioulnar deviation, in addition to obvious deformities and soft tissue swelling. Pinpoint areas of tenderness and correlate them to anatomic landmarks of the wrist to determine which structure may be injured and the best way to evaluate it radiographically (Figure 269-3).
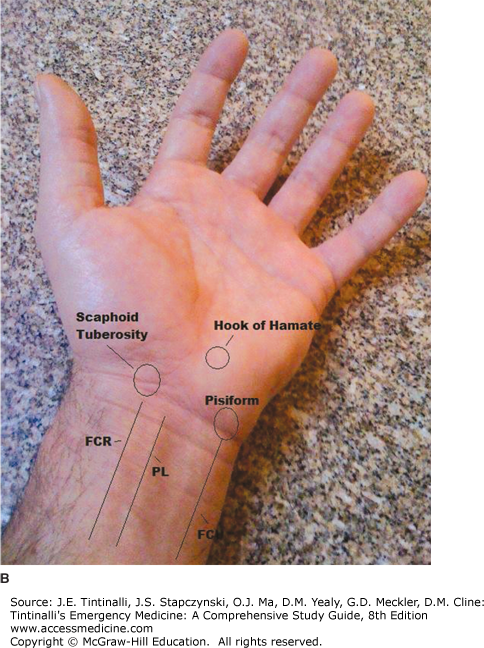
FIGURE 269-3.
Surface anatomy of the wrist. A. Dorsal aspect. B. Palmar aspect. APL = abductor pollicis longus; EPB = extensor pollicis brevis; EPL = extensor pollicis longus; FCR = flexor carpi radialis; FCU = flexor carpi ulnaris; LT = lunotriquetral joint; PL = palmaris longus; SL = scapholunate joint; STT = scaphotrapeziotrapezoid joint.
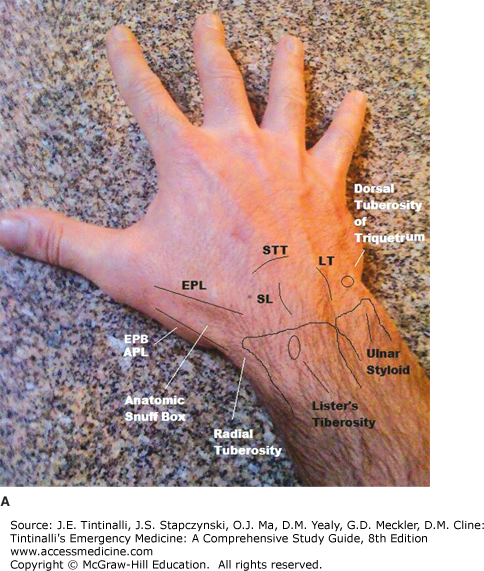
The most noteworthy landmark on the dorsum of the wrist is the anatomic snuffbox. The anatomic snuffbox is a triangle formed by the bony radial styloid at tis proximal base, the extensor pollicis brevis tendon at its radial aspect, and the extensor pollicis longus tendon at its ulnar aspect. Palpate the scaphoid within this triangle. Tenderness in this area may suggest a scaphoid fracture.10 The extensor pollicis longus tendon wraps around a bony prominence of the distal radius, known as Lister’s tubercle. The area immediately distal to this point marks the location of the scapholunate joint. Tenderness in this area suggests scapholunate ligamentous injury or lunate fracture.11 The scaphoid shift test can further assess scapholunate ligament injury. To perform the scaphoid shift test, place the wrist in ulnar deviation and apply pressure with your thumb over the scaphoid tuberosity. Then move the wrist from ulnar to radial deviation; in the event of ligament injury, you will feel a palpable “clunk.”
Immediately ulnar to the scapholunate joint is a palpable indentation in the center of the wrist. This is the location of the lunate and capitate, which are palpable as they rise out of this space during wrist flexion.11 Tenderness here may indicate lunate or triquetrolunate joint injury. The ulnar styloid is the bony prominence on the ulnar aspect of the wrist. The triquetrum and triangular fibrocartilage complex are located just distal to this prominence. Tenderness over the ulnar styloid may indicate ulnar styloid or triangular fibrocartilage complex injury. The ulnocarpal stress test can further evaluate the triangular fibrocartilage complex; apply a compression load to the wrist in ulnar deviation.7 Pain or clicking may indicate triangular fibrocartilage complex injury.
Pain with pronation and supination of the forearm may indicate distal radioulnar joint injury. The piano key sign, which is the ulnar head springing back when depressed while supporting the forearm in pronation, suggests distal radioulnar joint injury.11
The crease noted on the volar aspect of the wrist marks the location of the proximal carpal row (Figure 269-3). The scaphotrapezial joint is palpable at the base of the thenar eminence. The pisiform is the palpable bony prominence at the base of the hypothenar eminence. The hook of the hamate is palpable in the soft tissue distal and radial to the pisiform. Tenderness in these areas may require further evaluation than standard radiographic views.12
IMAGING
Clinical examination determines which radiographic views will best support a diagnosis. Standard views of the wrist include posteroanterior, lateral, and oblique views. These views are adequate in most cases, but other projections may be necessary for specific injuries.12,13
The key to interpreting the radiograph is to first ensure proper hand positioning, then identify specific features on each projection. On a properly positioned posteroanterior view, the distal radius and ulna should not overlap at their distal articulation, and the axis of the third metacarpal should parallel that of the radius. In addition to looking for disruption of the bony cortex, key elements on the posteroanterior view are illustrated in Figure 269-1.
On the posteroanterior view, three smooth arcs (Gilula lines) outline the articular surfaces at the radiocarpal and midcarpal joints. Two of these arcs are formed by the proximal and distal surfaces of the scaphoid, lunate, and triquetrum. The third arc is formed by the proximal articular surface of the capitate and hamate in the midcarpal joint. Any distortion of these lines implies a fracture, dislocation, or subluxation at the site.
The carpal bones fit together much like a jigsaw puzzle, with the pieces separated by a uniform 1- to 2-mm space. This space is increased or obliterated with ligament disruption, carpal instability patterns, or fracture/dislocations. This occurs most often around the lunate at the scapholunate and capitolunate joints.
The scaphoid has an elongated shape in its normal, palmarly flexed position. Fractures or ligament disruption may cause further palmar rotation, causing the scaphoid to appear shortened on the posteroanterior view. Injuries to the scaphoid also may obscure the scaphoid fat stripe, a linear or triangular radiolucent collection of fat distal to the radial styloid and parallel to the radial border of the scaphoid.
Unfortunately, incorrect positioning can produce overlap patterns that can be misinterpreted as pathologic. For example, radial deviation of the wrist causes normal physiologic rotation of the proximal carpal row, obliterating the capitolunate space. At the same time, the scaphoid that should appear elongated on the posteroanterior view appears shorter as it rotates palmarly and can be confused with a rotary subluxation of the scaphoid.
The radial styloid should project 8 to 18 mm beyond the distal radioulnar joint and create an ulnar inclination of 13 to 30 degrees on the PA view. Distal radius fractures can alter these measurements. At the distal radioulnar joint, the ulna and adjacent portion of the radius should be of equal length, forming a smooth articular surface, and the distal radius generally should articulate with at least half the lunate. The extrinsic ligaments along with the triangular fibrocartilage complex prevent ulnar translocation (migration of the carpal bones down the ulnar tilt of the radiocarpal surface).14 The lunate would have less contact and support from the radius if ulnar translocation were present. A shorter ulna (negative ulnar variance) also provides less support to the lunate and increases potential shear stress to the lunate, predisposing the lunate to injury.15
A properly positioned lateral radiograph is important for determining carpal alignment and degree of fracture angulation.12 The radius and ulna should completely overlap one another, and the radial styloid should be centered over the distal radial articular surface. The key elements are illustrated in Figure 269-4A.
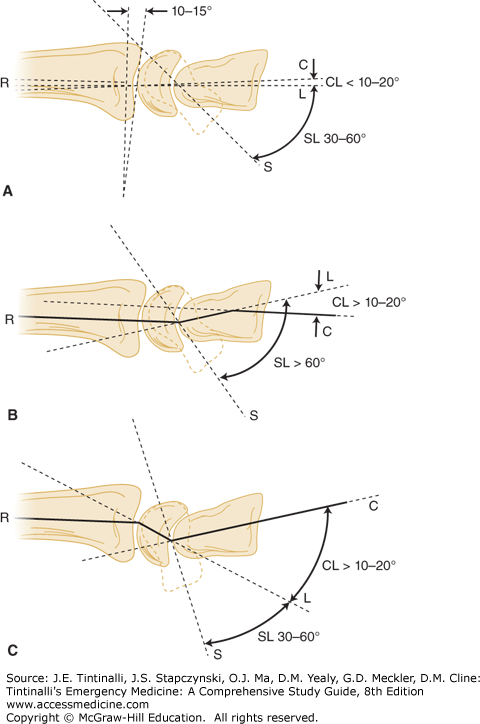
The axis of the radius, lunate, and capitate is collinear on the lateral view. If the articular surfaces of these bones were highlighted, they would appear as three consecutive C’s. This provides a simple radiographic assessment of wrist dislocation. Measurement of the capitolunate and scapholunate angles is a more precise assessment of carpal alignment. The axis of the capitate, lunate, and scaphoid runs through the center of their proximal and distal articular surfaces. The axis of the lunate and capitate should nearly overlap and form an angle that is <10 to 20 degrees. The scaphoid is normally palmar-flexed on the lateral view; its axis should form an angle between 30 and 60 degrees with the lunate. Deviation from either of these angles suggests ligament disruption and carpal instability patterns (Figure 269-4B and C).16
FIGURE 269-4.
A. Normal wrist. Axis of the radius (R), lunate (L), and capitate (C) are collinear (three C’s sign). The capitolunate (CL) angle is <10 to 20 degrees. The scapholunate (SL) angle is between 30 and 60 degrees. The radial volar tilt is 10 to 15 degrees. B. Dorsal intercalated segment instability. The lunate tilts dorsal and slides palmar, increasing the capitolunate angle. The scaphoid (S) tilts more palmar and increases the scapholunate angle. The axes of the radius, lunate, and capitate take on a zigzag pattern (yellow line). C. Volar intercalated segment instability. The lunate tilts palmar and the capitolunate angle increases, but the scapholunate angle is maintained. The zigzag pattern is in the opposite direction.
Fracture of the distal radius is the most common fracture in the wrist.14 Although a displaced fracture is the obvious deformity, the alteration of the normal volar tilt of 10 to 15 degrees of the distal radial articular surface has greater long-term consequences for wrist function, resulting in carpal misalignment and, subsequently, the instability patterns mentioned above.15
Other radiographic views profile specific areas of the wrist. Oblique views are performed in either partial pronation or supination, and project the scaphotrapezial joint or pisiform away from overlapping adjacent carpal bones. The scaphoid view is a cone-down posteroanterior view of the scaphoid in ulnar deviation. This position extends the normal flexed posture of the scaphoid so that the bone is projected lengthwise. This view may assist in detecting subtle fractures and is used whenever scaphoid injury is suspected.13 The carpal tunnel view is a tangential view through the carpal tunnel and is helpful in visualizing the pisiform and hook of the hamate. Motion studies are dynamic views in flexion, extension, and radial and ulnar deviation. These views examine carpal movement relative to one another, and stress the intercarpal ligaments for laxity, characterized by widening of the intercarpal space.17 Likewise, the grip compression or fist view is a stress view in the posteroanterior projection of the tightly clenched fist. The capitate is pushed into the proximal carpal row and forces the carpal bones apart if intrinsic ligaments are disrupted. CT is useful for defining fractures and dislocations, whereas MRI is useful for evaluation for both bony and soft tissue abnormalities such as occult fractures, avascular necrosis, and triangular fibrocartilage complex abnormality.17 Table 269-1 presents a summary of standard and supplemental wrist radiographs and the injuries they enhance.
| View | Injuries to Identify |
|---|---|
| Posteroanterior | Distal radius/ulna fractures, carpal bone fractures, ligamentous disruptions |
| Lateral | Radius/ulna fractures, lunate/perilunate dislocation, dorsal intercalated segment instability, volar intercalated segment instability |
| Scaphoid | Scaphoid fracture, scapholunate dissociation |
| Carpal tunnel | Pisiform and hamate fractures |
| Motion studies | Scapholunate or triquetrolunate instability |
| Grip compression | Scapholunate or triquetrolunate instability |
| CT | All fractures and dislocations |
| MRI | Occult fracture, avascular necrosis, soft tissue abnormality |
LIGAMENTOUS INJURIES
The lunate is located in the middle of the wrist, so it is not surprising that the majority of ligamentous injuries are centered on the lunate. Injuries usually result from forceful dorsiflexion of the wrist, most often from a fall on an outstretched hand. The various injuries occur sequentially depending on the degree of force and range from isolated tears to perilunate and lunate dislocations.18,19
The scapholunate ligament is the intrinsic ligament that binds the scaphoid and lunate. Because the scaphoid bridges the proximal and distal carpal rows, it is not surprising that the scapholunate ligament has a marked propensity for injury and is the most commonly injured ligament of the wrist. Injury most often is from a fall on an outstretched hand with impact on the thenar eminence.18 Patients complain of pain and swelling on the radial side of the wrist and often a “clicking” sensation with wrist movement. Examination reveals localized tenderness on the dorsum of the wrist in the area immediately distal to Lister’s tubercle. Ballottement of the scaphoid may also produce pain in this area.16
This injury is often referred to by the various radiographic appearances it may take. There are three different radiographic signs that may occur separately or in combination with one another (Figure 269-5A). Scapholunate dissociation is a widening of the scapholunate joint space of >3 mm on the posteroanterior view. If it is not apparent on routine views, a grip compression view or motion study may be necessary to demonstrate the abnormal gap (Figure 269-5B).19 These maneuvers are particularly helpful in identifying an incomplete tear of the ligament. Rotary subluxation of the scaphoid is another radiographic finding that often accompanies scapholunate dissociation. A torn scapholunate ligament can cause the scaphoid to tilt more palmar and increase the scapholunate angle to >60 degrees on the lateral view. On the posteroanterior view, the scaphoid tilts toward the observer so that it appears shorter as it is viewed more on its end. This causes the circular cortex of the bone to become more prominent and appear as a ring, known as the “cortical ring sign” (Figure 269-5A). A third radiographic abnormality is a carpal instability pattern known as dorsal intercalated segment instability (Figure 269-4B). The normal flexed posture of the scaphoid produces a flexion torque on the lunate that is counterbalanced by an extension torque from the triquetrum. When the scapholunate ligament is torn, this balance is disrupted. The lunate tilts dorsal from the unopposed extension torque from the triquetrum, whereas the scaphoid tilts more palmar (rotary subluxation of the scaphoid) because it has lost support from the lunate. The dorsal tilt of the lunate also causes a slight flexion tilt of the capitate. In the lateral view, the normal collinear arrangement of the axes of the capitate, lunate, and radius are replaced by a characteristic zigzag pattern. Both the scapholunate and capitolunate angles are increased. The concept of the proximal carpal row being the middle link or “intercalated segment” in this system, combined with the lunate’s pathologic dorsal tilt and zigzag pattern (Figure 269-5C), is how this abnormality came to be named dorsal intercalated segment instability.
FIGURE 269-5.
A. Scapholunate dissociation and rotary subluxation of the scaphoid. The scaphoid and lunate are separated by a gap of >3 mm (black arrow), and the scaphoid appears shorter from rotation with a dense ring, the “cortical ring sign” (white arrow). B. Grip compression view showing enhancement of scapholunate dissociation (arrow). C. Dorsal intercalated segment instability. Lateral view exhibiting dorsal intercalated instability with scapholunate dissociation. (See fig 269-4.)
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


