Ultrasound-guided view of the supraclavicular brachial plexus. The brachial plexus is located posterolateral to the subclavian (SC) artery. Note the close proximity of the first rib and pleura.
Infraclavicular block
Anatomy: The infraclavicular block provides anesthesia at the level of the cords of the brachial plexus, which surround the axillary artery deep to the pectoralis major and minor muscles. The cords are named for their positions relative to that artery: lateral, posterior, and medial. The axillary vein is usually located medial to the artery.
Landmarks: Coracoid process, deltopectoral groove, and clavicle.
Patient positioning: The patient’s arm can either be abducted (provides more distance between the probe and the clavicle for needle insertion [5]) or at their side.
Ultrasound-guided block technique: Although there are many approaches to this block, including the coracoid and vertical infraclavicular approaches, the ultrasound-guided lateral parasagittal approach will be described here [6]. Either a mid-frequency curvilinear probe (larger patients) or a high-frequency linear probe (thin patients) may be used but a smaller footprint probe will afford more room between the clavicle and the probe for needle insertion. Place the probe in the parasagittal plane beneath the clavicle and approximately 2 cm medial to the coracoid process to obtain a transverse view of the axillary artery and surrounding cords (Figure 33.2).
Using the short axis, in-plane approach, the needle should be inserted from cephalad to caudad. The needle should pass lateral to the lateral cord and aim between the posterior cord and the axillary artery (approximately the six o’clock position relative to the artery). In this positioning, local anesthetic should ideally disperse in a “U”-shape around the artery, spreading both to the lateral and medial cords. If combined with nerve stimulation, a posterior cord twitch (wrist or hand extension) should be sought [7].
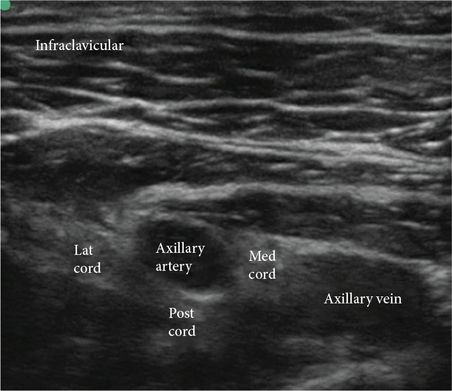
Ultrasound-guided view of the infraclavicular brachial plexus. Transverse view of the axillary artery and surrounding cords: lateral, medial, and posterior.
Axillary
Anatomy: In the axilla, the brachial plexus has divided into terminal branches: the median, radial, musculocutaneous, and ulnar nerves. The axillary nerve has already branched off the posterior cord and will not be blocked with this technique. The median, radial, and ulnar nerves are in an axillary sheath along with the axillary artery. The musculocutaneous nerve runs outside of the axillary sheath, pierces the coracobrachialis muscle and descends between the biceps and coracobrachialis muscles.
Landmarks: Axillary artery, axillary fossa.
Patient positioning: Supine with the operative arm abducted 90 degrees.
Technique: A variety of techniques exist for the axillary block including transarterial, nerve stimulator, and ultrasound-guided. The ultrasound-guided technique will be described here.
Ultrasound-guided block technique: Using a high-frequency, linear probe and a short axis, in-plane technique, the US probe should be placed proximally in the axilla, at the junction of the pectoralis and the biceps muscles in a transverse orientation to the arm. Identify the axillary vessels, surrounding nerves and muscles (biceps, triceps, and coracobrachialis). The typical orientations of the nerves in relation to the axillary artery are as follows.
The median nerve is cranial and lateral to the artery; the ulnar nerve is caudal/medial to the artery (between the artery and the axillary vein); and the radial nerve is posterior to the artery (Figure 33.3). The axillary vein is also found caudal/medial to the artery, but is often compressed by the US probe so that it is not visualized on imaging. A nerve stimulator may be useful in identifying each nerve in conjunction with ultrasound. A 5 cm, 22G insulated needle should be directed in the cranial to caudal orientation in plane with the US probe. The musculocutaneous nerve can be found by moving the US probe more cephalad and distal. It may appear as a hypoechoic oval surrounded by hyperechoic fascia in the body of the coracobrachialis or between the biceps and coracobrachialis muscles. Between 5 and 8 ml of local anesthetic should be injected around each nerve.
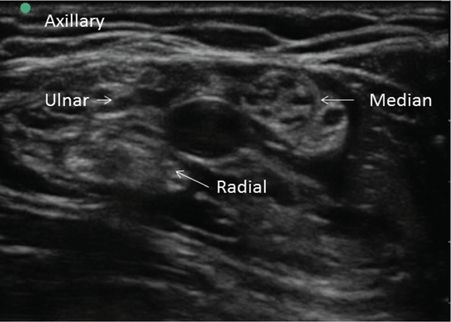
Ultrasound-guided view of the axillary brachial plexus. Transverse view of the axillary artery and the surrounding terminal branches: ulnar, median, and radial nerves.
Useful tips
A total of 20 to 30 ml of local anesthetic is appropriate for most of these blocks.
If the surgeon is planning on using a tourniquet, an intercostobrachial block may be required to avoid tourniquet pain. This nerve is derived from the T2 nerve root and innervates the skin of the axilla and the medial aspect of the upper arm. It can be blocked by infiltrating a subcutaneous ring of local anesthetic in the proximal axilla from the insertion of the pectoralis muscle to the latissimus muscle insertion.
2. Analyze the benefits, drawbacks, side effects, and complications of each block
Benefits, drawbacks, side effects, and complications of supraclavicular, infraclavicular, and axillary blocks.
| Block type | Supraclavicular | Infraclavicular | Axillary |
|---|---|---|---|
| Benefits | Blocks mid-humerus to hand “Spinal” of the arm | Blocks mid-humerus to hand Bilateral blocks possible Ideal catheter site | Blocks forearm to hand Bilateral blocks possible No risk of respiratory compromise |
| Drawbacks | Potential pneumothorax Not appropriate for bilateral blocks | Caution in coagulopathy | Not ideal catheter location Abduction of the arm is necessary |
| Side effects | Horner’s syndrome Hoarseness Diaphragmatic paralysis | None | None |
| Complicationsa | Pneumothorax Arterial puncture | Pneumothorax (rare) Arterial puncture | Arterial puncture |
a Block-specific complications; other complications include local anesthetic toxicity, nerve injury, bleeding, and block failure.
Supraclavicular
Benefits: Anesthesia or analgesia for surgery on the upper extremity from the mid-humerus to the hand. This technique can provide a dense block after a single injection due to the compact nature of the trunks at this location, and has been referred to as the “spinal” of the upper extremity.
Drawbacks: Potential for pneumothorax (1–5% pre-US) [8].
Side effects: Phrenic nerve blockade in 50% of patients [9], recurrent laryngeal and stellate ganglion blockade.
Complications: Bleeding, infection, nerve injury, or pneumothorax (<1% with US).
Infraclavicular
Benefits: Anesthesia or analgesia for surgery on the upper extremity from the mid-humerus to the hand. For some patients, the infraclavicular block may be advantageous over the axillary block, as there is no need to abduct the arm or identify the musculocutaneous nerve. Compared with the supraclavicular approach, phrenic nerve blockade is rare [9]. The infraclavicular location is also an ideal place for continuous catheter placement, with superior analgesia when compared to supraclavicular indwelling blocks [10].
Drawbacks: This block is considered a deep, peripheral nerve block and should be used with caution in patients who are anticoagulated or having bleeding abnormalities. It can also be technically difficult in obese patients.
Side effects: None.
Complications: Bleeding, infection, and nerve injury. There have been case reports of phrenic nerve blockade from the infraclavicular block, though rare [11]. A retrospective review of 1,138 patients who received US-guided infraclavicular blocks revealed a 99.3% success rate with 0.7% arterial puncture and no cases of pneumothorax, local anesthetic toxicity, or nerve injury [12].
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


