CHAPTER 18 Vertical infraclavicular block
Clinical anatomy
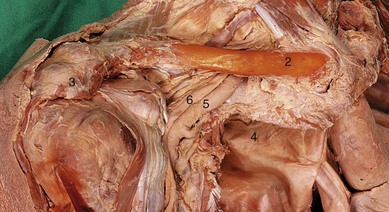
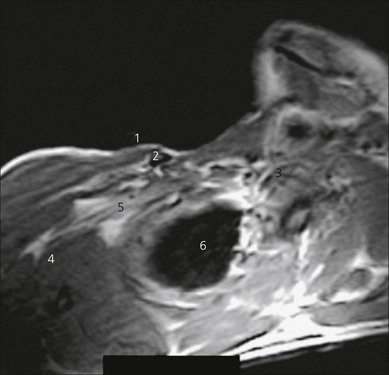
The brachial plexus passes behind the clavicle to enter the axilla. Here it lies laterally to the subclavian vessels and dome of the lung (Fig. 18.1). Above the clavicle, the trunks have formed divisions that continue to form the cords of the plexus in the axilla.
Surface anatomy
Important bony landmarks are the clavicle, anterior aspect of the acromion, the suprasternal notch, and the spine of the scapula. The distance between the suprasternal notch and anterior aspect of the acromion is measured and divided equally to find the needle insertion point, inferior to the clavicle (Fig. 18.2). Recent studies have shown that the optimal site in females may be 0.8 cm lateral to the midpoint. In adults, this distance is usually greater than 17 cm. A healed fractured clavicle will change the relations of this insertion point and is thus a relative contraindication for performing this block without ultrasound.

The needle insertion point is lateral to the apex of the lung (Fig. 18.3). This can be confirmed by palpating the subclavian artery both above the clavicle and medial to the needle insertion point.
Sonoanatomy
The ultrasound-guided infraclavicular technique is performed over the pectoral region. In view of the increased depth at which the brachial plexus is found at this level with respect to other techniques, the ultrasound transducer should be of lower frequency (4–7 MHz). Scanning is performed laterally in proximity to the coracoid process (Fig 18.4). The ultrasound transducer (curvilinear, held in a sagittal orientation) is placed near the lower edge of the clavicle, and a transverse view (parasagittal plane) of the axillary artery and vein is obtained (Fig 18.5). A good alternative is to use a small curved transducer for infraclavicular scanning since it provides a wider field of view and more space for needle insertion. However, phased array or linear transducers can also be used. Care should be used not to apply too much downward pressure on the transducer, which may occlude the axillary vein. The Doppler options facilitate identification of the vascular structures.

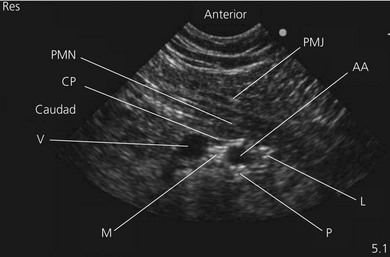
Perform a systematic anatomical survey from superficial to deep. The pectoralis major and minor muscles are most superficial and easily identified. Identify the axillary artery and vein deep to the pectoralis minor muscle. The vein is almost always caudad to the artery. Look for hyperechoic nerve structures around the axillary artery. Hyperechoic density posterior to the axillary artery can be due to ‘acoustic enhancement’, an artifact generated when the ultrasound beam crosses a vessel with little acoustic impedance. Angle (tilt) the transducer slightly in the parasagittal plane to check if this hyperechoic structure stays in the same location. If it does not, this is not likely to be a nerve structure. The pleura or chest wall is identified as a hyperechoic fine line outlining the anechoic lung tissue if the transducer is moved medially. It can be seen to move with respiration. The plexus is usually found at a depth of 2–6 cm. The cords of the plexus are located adjacent to the artery in medial, lateral and posterior positions (Fig 18.5). Upper limb position does influence these relationships. Arm abduction to 90° will bring the three cords closer together and will enhance nerve visualization. The pectoralis major, pectoralis minor muscles and clavipectoral fascia are visualized and further identified by appropriate resisted movements.









