CHAPTER 30 Popliteal block
Clinical anatomy
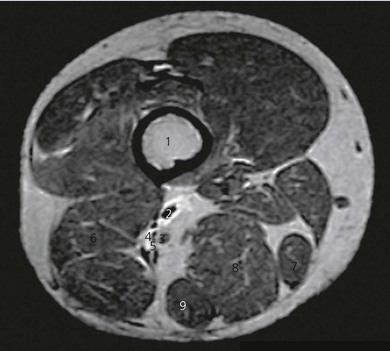
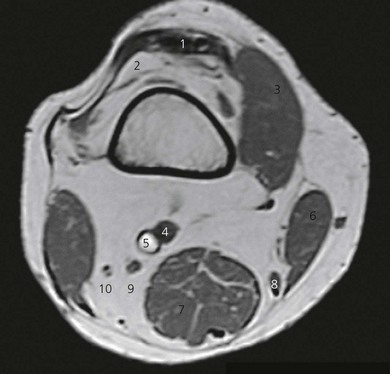
The popliteal fossa is defined as the space between the skin, the femur anteriorly and the biceps femoris muscle laterally, the semitendinosus and semimembranosus muscles medially, and inferiorly by both heads of the gastrocnemius (Figs 30.1 and 30.2). The space is mostly filled with fat and contains in its anterolateral aspect the popliteal vessels and nerves. The sciatic nerve is formed from roots L4 to S2 (and occasionally S3) and consists of two distinct divisions – the tibial and common peroneal nerves – which share a common epineural sheath from their origin to the popliteal fossa. The two nerves innervate the entire leg below the knee except for the anteromedial leg and foot, which are innervated by the saphenous nerve (L2, 3, 4).


The sciatic nerve branches in the region of the distal thigh (Fig. 30.3), anywhere between 4 and 13 cm above the popliteal crease, although occasionally they can run as two separate nerves from the sciatic foramen. The tibial nerve is the larger of the two branches and runs parallel and slightly lateral to the midline. Inferiorly, it passes between the heads of the gastrocnemius muscle. The common peroneal nerve runs laterally along the medial aspect of the biceps femoris muscle. After bifurcation, the tibial nerve immediately gives off the sural nerve, which innervates the lateral aspect of the foot. The common peroneal nerve also gives off a sural communicating nerve (Fig. 30.4), and once it is below the head of the fibula it divides into superficial and deep peroneal nerves. The nerves lie more superficial and lateral to the popliteal vessels in the popliteal fossa and about midway between the skin and the posterior aspect of the femur.
Surface anatomy
The main landmarks for the lateral popliteal block include the superior aspect of the patella and a muscular groove between the biceps femoris and vastus lateralis muscles (Fig. 30.5). Identification of this groove is difficult in obese patients and should be mastered prior to procedure. This is easily felt when patients flex their leg against resistance.

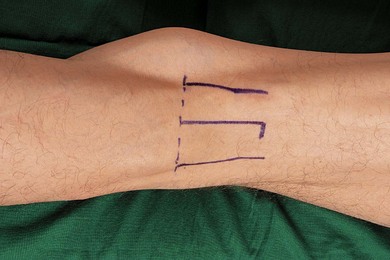
The main landmarks for the posterior popliteal block include skin crease of the knee joint and biceps femoris muscle laterally, and semimembranosus muscle medially (Fig. 30.6). The patient can be asked to flex the leg to identify the margins of the popliteal fossa. Absence of bony landmarks with the posterior approach increases the learning curve with this approach.
Sononatomy
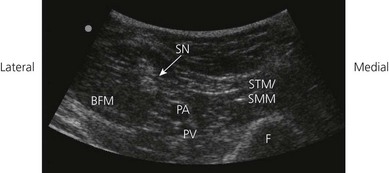
Using a transverse transducer orientation, perform a systematic anatomical survey of structures from superficial (skin) to deep and from medial to lateral in the popliteal fossa (Fig. 30.7). First identify the femur, which is deep and casts a bony shadow. Next, identify the pulsatile popliteal artery that is superficial to the femur (Fig. 30.8). If it is not visible, scan distally towards the popliteal crease where the popliteal artery is more superficial. The popliteal vein may or may not be visible (collapsed by transducer pressure). Note the muscle groups medially (semitendinosus and semimembranosus muscles) and laterally (biceps femoris muscle; Fig. 30.8). The hyperechoic sciatic nerve in this location is always superficial to the femur and lateral to the popliteal artery (Fig. 30.8). If the sciatic nerve is not easily visible, angle the transducer and aim the beam caudally towards the foot (Fig. 30.9). This will bring the nerve into view once the angle of incidence is approximately 90° to the nerve. Scan the region proximally and distally to assess nerve anatomy. Position the transducer in a location where the sciatic nerve is clearly visualized as a single nerve before its bifurcation. Nerve visualization is significantly improved once local anesthetic is injected, due to enhanced contrast between the hyperechoic nerve and the hypoechoic fluid collection.

Figure 30.7 The ultrasound transducer is positioned in the popliteal fossa with a transverse orientation.

Technique
Landmark-based approach
Lateral approach
The patient is placed supine, with the lower limb in the neutral position. The feet should be extended beyond the edge of the table in order to better discern the response to nerve stimulation (Fig. 30.10). A small sandbag underneath the knee or a pillow under the thigh facilitates the technique. The upper border of the patella is identified and a line is drawn vertically downward to the patient trolley. The groove between the lateral border of vastus lateralis and the biceps femoris tendon is identified. The intersection of the two lines is the needle insertion point.
< div class='tao-gold-member'>







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


