CAPNOGRAPHY
CO2 identified in expired gas by spectrographic properties (using IR, Raman, or mass spectroscopy)
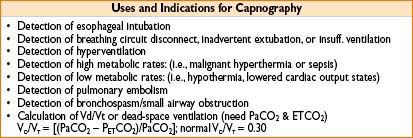
Hazards of Capnography:
• Old in-line IR detectors can heat up, causing facial thermal injury
• May fail to detect disconnection if machine disabled by secretions, or alarms disabled
CAPNOGRAPHS
Figure 8-2. Normal capnograph (normal expired CO2 waveform).
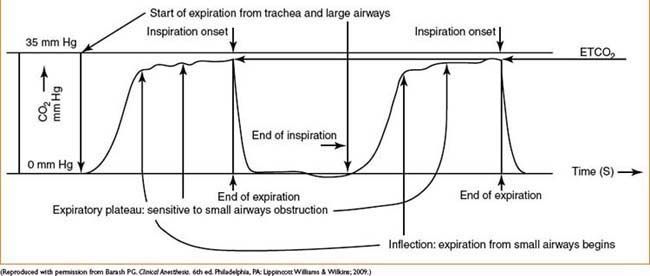
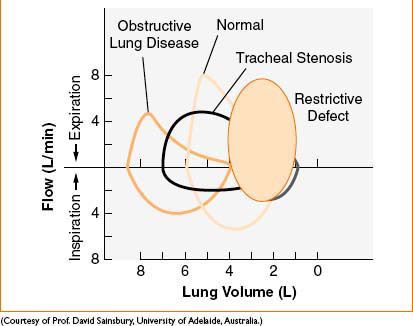
Figure 8-3. Normal and abnormal flow volume loops.
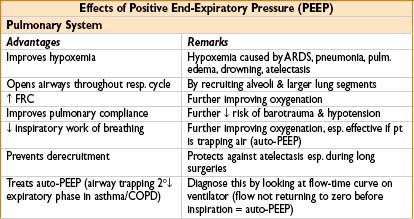
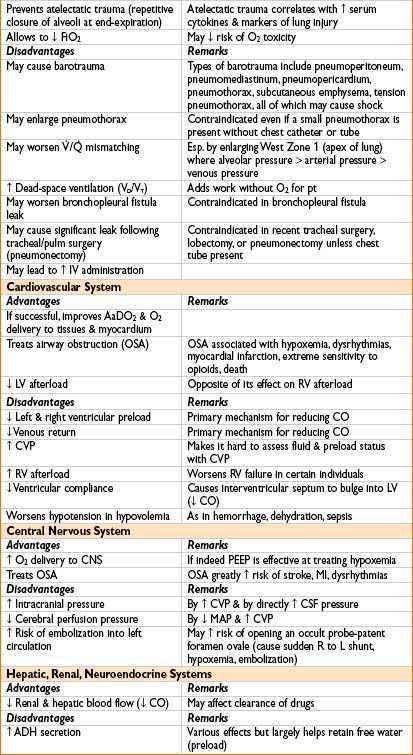
MECHANICAL VENTILATION: PROTECTIVE STRATEGIES
Current Strategies to Prevent Volutrauma, Barotrauma, Atelectrauma, Tracheal Ischemia & O2 Toxicity
• Alveolar overdistention (volutrauma), rather than excessively ↑ airway pressure (barotrauma), may be more injurious to lung
• Smaller tidal volumes (6 mL/kg) are recommended with greater respiratory rate
• Higher PaCO2 levels allowed (permissive hypercapnia) in treating acute lung injury & ARDS
Specific Settings
• TV 6 mL/kg (prevents volutrauma: trauma from overdistention of alveoli)
• Plateau pressure <30 cm H2O (prevents barotrauma: trauma from excessive press.)
• PEEP >6–10 cm H2O (prevents atelectatic trauma: repeated alveolar closure at end-expiration)
• FiO2 <50% to prevent O2 toxicity
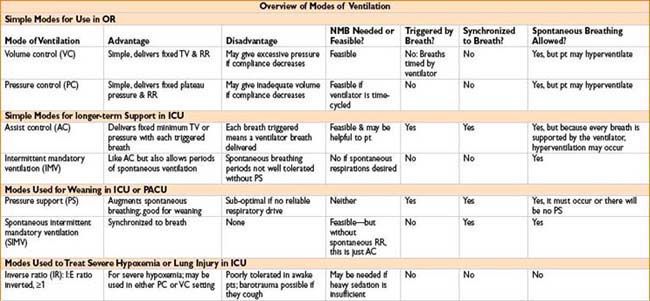
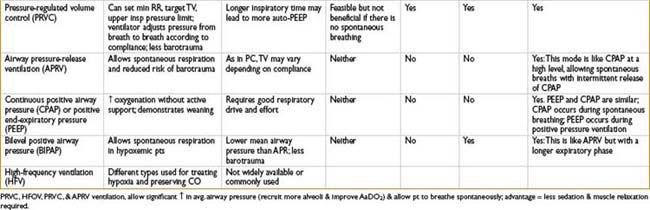
BIPAP VS. CPAP
• CPAP = delivery of continuous positive air pressure throughout respiratory cycle
• BiPAP = two levels of positive air pressure, inspiratory (triggered by insp effort) & expiratory (present throughout the rest of the respiratory cycle) (expiratory pressure is lower to facilitate exhalation)
DISCONTINUING MECHANICAL VENTILATION
SIMV Plus PS is a Common Weaning Mode in Many ICUs
• Start with full support (IMV ≈ 10), plus PS 10–15 cm H2O, PEEP 5–10
• Decrease by 1–2 breaths per minute till IMV = 0
• Now wean PS 1–2 cm H2O at a time until PS/PEEP is 10/5 or 5/5 cm H2O or lower (for more deconditioned pts, you may need to go as low as PS/PEEP = 2/5)
• At the same time gradually reduce FiO2 according to SaO2 or PaO2 (more sensitive to oxygenation changes)
< div class='tao-gold-member'>









