Acute
Chronic
Neck and Upper Extremity
Carotid Artery Dissection
Subclavian or Axillobrachial Atherosclerosis
Vertebral Artery Dissection
Hemodialysis-Associated Steal Syndrome
Thoracic Outlet Syndrome (arterial or venous)
Thoracic Outlet Syndrome (neurogenic)
Acute Arterial Thromboembolism
Raynaud’s Phenomenon
Upper Extremity Deep Vein Thrombosis
Vasculitis (scleroderma, lupus)
Hypothenar Hammer Syndrome
Chest and Abdomen
Acute Aortic Dissection
Chronic Aortic Dissection
Aortic Aneurysm (thoracic or abdominal)
Aortic Aneurysm (thoracic or abdominal)
Acute Mesenteric Ischemia
Chronic Mesenteric Ischemia
Lower Extremity
Lower Extremity Deep Vein Thrombosis
Postthrombotic Syndrome
Acute Arterial Thromboembolism
Venous Insufficiency/Reflux—Varicose Veins
Popliteal Artery Aneurysm with Thrombosis
Aortoiliac or Femoropopliteal Atherosclerosis
Exertional Compartment Syndrome
Popliteal Entrapment Syndrome
A general description of the various surgical and endovascular procedures employed by the vascular specialist for the treatment of pain by anatomic region, as well as the outcomes of these interventions will be reviewed in this chapter. The role of the rehabilitation specialist in the management of patients with pain of vascular origin begins with postoperative rehabilitation after vascular intervention. It is important for the rehabilitation specialist to be able to recognize acute pain syndromes and postoperative complications, which should prompt referral to a vascular specialist.
Neck and Upper Extremity
Neck pain resulting from spontaneous or traumatic dissection of the extra-cranial carotid or vertebral arteries is rare but may account for up to 20% of ischemic strokes. A large population-based study found the incidence of spontaneous extra-cranial internal carotid artery dissection was 1.72 per 100,000 and 0.97 per 100,000 for vertebral artery dissection [1]. The mainstay of treatment for extra-cranial internal carotid or vertebral artery dissection, according to the AHA/ASA guidelines, is anticoagulation for 3–6 months.
Surgical reconstruction or stent placement is reserved for patients with persistent symptoms despite anticoagulation or antiplatelet therapy [2]. Surgical reconstruction for carotid artery dissection was associated with a 10% postoperative stroke rate and a 40% rate of cranial nerve damage at long-term follow-up in one series [3]. The use of endovascular stents effectively eliminates the risk of cranial nerve injury associated with open repair, without any difference demonstrated in the postoperative stroke rate [4].
Stroke rehabilitation may be initiated within 48–72 h after carotid endarterectomy. Patients may have some tenderness on neck rotation for the first 1–2 weeks, so driving in this time period is not recommended. The operative vascular surgeon should be consulted immediately if sudden neck swelling is observed during rehabilitation. After carotid stent placement, rehabilitation may begin within 24–48 h after intervention without restriction in most cases.
Dual antiplatelet therapy is required for the first 3 months after stent placement, so the assessment of fall risk is essential, prior to discharge home, since a fall with head trauma in these patients may be devastating. The interventionist should be consulted immediately if a sudden, expanding, erythematous, or necrotic groin hematoma is observed. Evaluation in the emergency department should be pursued if any new symptoms of transient ischemic attack or stroke occur during rehabilitation after endarterectomy or stent placement.
Thoracic Outlet Syndrome (TOS ) is due to compression of the brachial plexus, subclavian artery, or subclavian vein by fibrous bands to the first rib, or by a cervical rib where these structures exit the thoracic cavity. The syndrome frequently presents with pain. The nonoperative management options for the syndrome should be familiar to the rehabilitation specialist, as more than 80% of cases are neurogenic and treatment is conservative.
Operative treatment is reserved for the <5% of patients who present with arterial or venous TOS, or for those patients who have failed conservative measures aimed at alleviating symptoms for neurogenic TOS. Treatment involves first rib resection via an axillary, supraclavicular, or thoracoscopic approach. Patients who present with arm pain and upper extremity deep vein thrombosis, due to compression of the subclavian vein (Paget–Schroetter syndrome), may be treated with venous thrombolysis and/or thrombectomy prior to rib resection.
Arterial TOS can manifest as acute or chronic extremity pain, absence of pulse, or distal embolization, and may have associated rudimentary or cervical ribs. An arterial reconstruction surgery may be indicated at the time of rib resection if aneurysmal degeneration, stenosis, or occlusion of the subclavian artery has developed. First rib resection is associated with positive long-term outcomes in 95% of patients treated for all indications [5].
Occupational therapy can generally be resumed within 3–5 days after surgery, but sports and strenuous activity should be delayed for at least 2 weeks. Edema is usually successfully managed with arm elevation. While complications are rare, the operative surgeon should be contacted if patients complain of acute pain or if loss of pulses in the arm is noted on exam.
Upper extremity pain of arterial origin may be due to atherosclerotic disease, although this is uncommon. More frequently observed is hemodialysis-associated steal syndrome, which affects up to 10% of patients receiving hemodialysis with an arteriovenous fistula or graft. As the prevalence of end-stage renal disease continues to rise, prevalence of this syndrome will likely also rise in the rehabilitation setting.
Classically, the syndrome results from excess blood flow through the fistula or graft, which ‘steals’ blood supply from the distal extremity. It may also result from arterial stenosis of the inflow artery or from failure of forearm collateral circulation to develop after access creation. Symptoms can range from digital pain or paresthesia to ulceration and gangrene. Prompt recognition is essential for prevention of permanent ischemic nerve damage or need for amputation. A vascular surgeon should be consulted urgently for any patient with an arteriovenous fistula or graft who complains of ipsilateral hand numbness or decreased range of motion, or if ischemic changes are noted in the fingertips on exam.
While ligation of the arteriovenous access remains the “gold standard” treatment for hemodialysis access-associated steal syndrome, a number of surgical procedures have been devised to correct the underlying pathophysiology, while preserving the dialysis access for use. Banding involves focally narrowing the graft, either at the arterial anastomosis or mid-portion, in order to reduce flow through the conduit. Additional strategies include the DRIL procedure (Distal Revascularization and Interval Ligation), RUDI procedure (Revision Using Distal Inflow), and PAI procedure (Proximalization of Arterial Inflow) [6].
A large retrospective review found that, with the exception of ligation where the access is sacrificed, these procedures are associated with >90% hemodialysis access preservation. Improvements in steal symptoms were demonstrated in >90% of patients for all procedures except banding (75%). Ligation and DRIL were associated with the lowest 30-day complication rates (8% and 7%, respectively), whereas more than one-third of patients who underwent banding, RUDI, and PAI had complications ranging from infections, hematoma formation, continued steal, or access thrombosis within 30 days of the procedure [7]. Patients may generally return to usual activity within 3–5 days after these procedures. Occupational therapy may be indicated to rehabilitate the previously ischemic hand.
Upper extremity pain of venous origin is typically associated with upper extremity deep vein thrombosis (DVT), with an incidence in the general population of 2 per 100,000 persons per year. Upper extremity DVT may be secondary to venous thoracic outlet syndrome, indwelling central catheters, malignancy, and/or hypercoagulable disorders. In addition to therapeutic anticoagulation and limb elevation, catheter-directed thrombolysis may be utilized to treat postthrombotic pain in the acute setting. This involves inserting a catheter into the thrombus and infusing thrombolytic agent directly into the clot to dissolve it, with or without the adjunctive use of mechanical thrombectomy to break up the clot (Fig. 60.1). At long-term follow up, catheter-directed thrombolysis for upper extremity DVT can be associated with complete resolution of postthrombotic syndrome in up to 80% of patients [8]. Patients will often require arm elevation, while at rest, to resolve the edema from upper extremity DVT, but rehabilitation may continue without restriction.
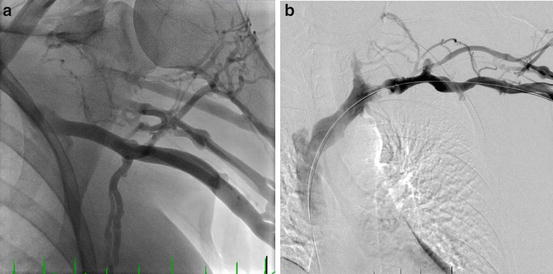
Fig. 60.1
Upper extremity catheter-directed thrombolysis. (a) Angiogram prior to thrombolysis demonstrating acute thrombosis of the subclavian vein. (b) Angiogram after thrombolysi s, with subclavian vein recanalization demonstrating underlying vTOS
Chest and Abdomen
Chest pain of noncardiac vascular origin is most commonly encountered acutely in patients with thoracic aortic dissection, or more chronically in patients with aneurysmal degeneration of the thoracic aorta, with an incidence of approximately 3 and 6 per 100,000 persons per year, respectively [9, 10]. Prompt surgical aortic replacement is necessitated for patients with “Type A” aortic dissections involving the ascending aorta and/or aortic arch. This repair is performed by a thoracic surgeon via a median sternotomy approach and requires total cardiopulmonary bypass with hypothermic circulatory arrest. Surgery of this type is associated with an in-hospital mortality rate as high as 30%. Furthermore, 15% of survivors have a postoperative course complicated by a neurologic deficit (stroke or paraplegia) [11].
For patients with “Type B” dissections involving the descending aorta, surgical or endovascular treatment is indicated emergently for rupture, mal-perfusion (visceral, spinal, or limb), or persistent pain. Patients with known type B dissections, who are being cared for in the rehabilitation setting, should be transferred to an emergency department immediately if sudden hypotension; paraplegia; or severe pain in the chest, back, abdomen, or lower extremities develops.
Open surgery involves a left posterolateral thoracotomy, can lead to profound hemodynamic shifts from aortic cross-clamping, and often requires significant postoperative rehabilitation. Thoracic endovascular stent graft placement (Fig. 60.2) can be performed either percutaneously or via minimal groin incisions, minimizes intraoperative hemodynamic changes, and significantly reduces postoperative pain and recovery time, when compared to open repair. In a meta-analysis, the endovascular approach for Type B dissection is associated with a significantly lower 30-day mortality, when compared to open repair (11% vs. 35%, respectively); however, there is no significant difference in the rates of postoperative paraplegia (9% vs. 8%, respectively) [12].
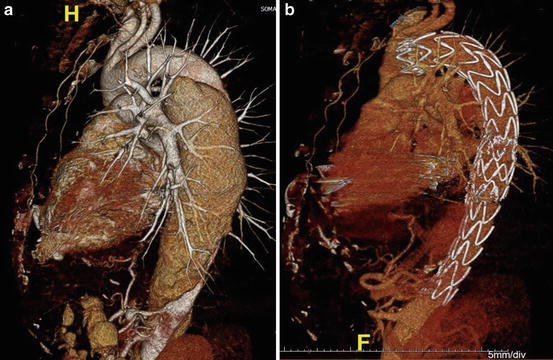
Fig. 60.2
Endovascular repair of thoracic aortic dissection. (a) CT 3D reconstruction demonstrating Type B dissection with aneurysmal degeneration. (b) CT 3D reconstruction after endograft placement demonstrating exclusion of the false lumen
The same surgical and endovascular approaches are employed in the treatment of thoracic aortic aneurysms in an elective setting. Results from the Nationwide Inpatient Sample demonstrate low overall operative mortality (4.5%) for both procedures, with decreased odds of postoperative neurologic, cardiac, and respiratory complications in the thoracic endograft group [13]. In uncomplicated cases, rehabilitation may begin 3–5 days postoperatively. In complicated cases, patients may be severely debilitated by the time they are medically ready for rehabilitation. Postoperative cardiopulmonary rehabilitation is often required after open repair. In patients with postoperative paraplegia, partial or complete recovery of neurologic function with intensive rehabilitation can be expected in most patients.
Related posts:
 Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
 Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
 Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


