(1)
Chennai Breast Centre, Chennai, India
Breast cancer is a heterogeneous disease with a varied clinical outcome, underscoring the need for the use of reliable predictive and prognostic biomarkers. Prognostic markers help in estimating clinical outcome while predictive markers are required for optimal therapeutic decision making. Testing for steroid hormone receptors and HER2 oncogene have been, for many years, the mainstay of breast cancer management, both for prognostication and in predicting response to hormonal therapy, anti-HER2 therapy, and chemotherapy. Ki67, a key proliferative marker, has in recent times, evoked much interest due to its moderate prognostic value and its role in neoadjuvant therapy. Recent molecular advances have also identified several other single gene products as well as, more critically, multigene signatures for breast cancer which can provide further prognostic and predictive information, to help fine-tune treatment strategies.
Steroid Hormone Receptors
The steroid hormones estrogen and progesterone regulate ductal growth and alveolar development, respectively, in the normal breast; they also play a critical role in breast cancer development and progression. Their actions are mediated by binding with hormone receptors. Estrogen and progesterone receptors status is a weak prognostic marker of disease outcome but is strongly predictive of response to hormonal therapy, such as tamoxifen-based therapy. Consequently, robust and quality-controlled assays with standardized interpretation are required to accurately guide therapeutic decisions. Biochemical methods were initially used, but immunohistochemistry on formalin-fixed paraffin-embedded tissue is currently the method of choice to assess hormone receptor levels in breast cancers.
The American Society of Clinical Oncology (ASCO) and the College of American Pathologists (CAP) have recently published guidelines recommending that ER and PR should be tested on all newly diagnosed invasive breast cancers and on local and distant recurrences as appropriate. These guidelines also provide recommendations on standardization and validation of IHC assays with an aim to improve the accuracy and reproducibility of hormone receptor testing.
Estrogen Receptor
Estrogen receptors are nuclear transcription factors that bind to the hormone estrogen and regulate the growth and development of normal mammary tissue. The estrogen signaling pathway follows the standard steroid receptor mechanism. Estrogen diffuses through the cellular membrane and binds monomeric ER with resultant receptor dimerization. The ligand/receptor complex then binds to elements in the promoter regions of estrogen-responsive genes enhancing transcription. Two homologous ER isoforms are present, ERalpha and ERbeta, encoded by two separate genes, ESR1 and ESR2, respectively. The pathophysiologic role of ERb is currently uncertain, with no evidence to support evaluation of ERb.
Estrogen receptors alpha (ERα) are expressed in approximately 70–80 % of breast cancer cases; binding of Estrogen to ERα induces tumor growth in most ERα-positive breast cancer cell lines and also inhibits apoptosis of breast cancer cells by upregulating Bcl-2 expression.
ER protein was first characterized in the mid-1960s while the first reports of the prognostic and predictive properties of ER were published in the early 1970s. Ligand-binding assays, which required homogenization of fresh frozen tissue, were initially used to quantify estrogen receptors; monoclonal antibodies to ER with quantification by enzyme immunoassays were introduced in the 1980s. Immunohistochemistry for hormone receptor–specific antibodies was initially performed on frozen tissue; newer antibodies and refinements in antigen retrieval methods developed in the early 1990s permitted the use of formalin-fixed and paraffin-embedded tissue (Fig. 26.1). IHC is now almost universally accepted as the method of choice as it is inexpensive, routinely available, and as it is performed by direct visualization of tumor, allows estimation even in cases with scanty tumor tissue.
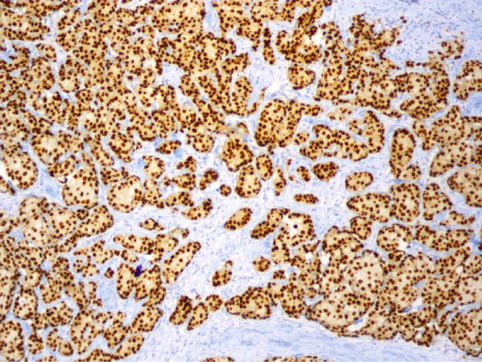
Fig. 26.1
ER positive (quick score 8/8): strong nuclear staining of more than 2/3 of tumor nuclei
Progesterone Receptor
Progesterone receptor (PR) is also frequently measured for the management of breast cancer (Fig. 26.2). Like ER, PR was initially assessed by ligand binding assays but is now measured largely by IHC. PR protein also exists as two receptor isoforms, A and B, which are products of the same gene. The gene encoding for PR is estrogen dependent and, thus, PR expression might serve as an indicator of the integrity of the ERα pathway and help to predict response to hormonal therapy.
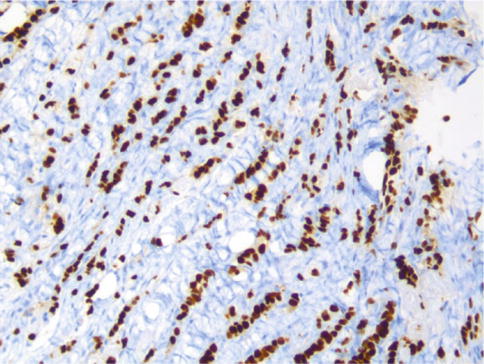
Fig. 26.2
PR positive (quick score 8/8): strong nuclear staining of more than 2/3 of tumor nuclei
Improving Standards of ER, PR Reporting
There is a need to improve standards of IHC testing and reporting of ER and PR status as there is evidence suggesting that up to 20 % of ER/PR tests are inaccurate, primarily due to inconsistencies in pre-analytic variables and in interpretation criteria. False negatives could have serious implications for patient management, while false positives may result in unnecessary overtreatment.
The recently published ASCO/CAP guidelines for ER and PR testing by IHC serve to address these issues by defining two key areas:
An optimal testing algorithm for determining ER and PgR status
Strategies to ensure ideal performance, interpretation, and reporting of established assays
Optimal Testing Algorithm
The initial clinical validation studies correlating Estrogen and progesterone receptor status with response to endocrine therapy in patients were done with LBAs; the evidence from a number of published studies led to receptor testing with LBAs being established, in 1974, as the gold standard. Several studies directly comparing the abilities of ERα testing by LBA and IHC have demonstrated that IHC is equivalent or even better in predicting response to hormone therapy as IHC testing results as low as 1 % positive-staining carcinoma cells can be associated with a significant clinical response.
Strategies to Ensure Optimal Performance, Interpretation, and Reporting of Established Assays
Preanalytic Standardization: Tissue Handling
There is progressive loss of activity of labile molecules, such as RNA, DNA, and proteins, after surgical interruption of blood flow, due to tissue ischemia, acidosis, and enzymatic degradation. The warm ischemia time (time from the interruption of the blood supply to the tumor to the excision of the tissue specimen) and cold ischemic time (time from excision to the initiation of tissue fixation) are, therefore, critical parameters which need to be standardized. The tissue must be placed in fixative within an hour of removal; both the time of collection and the time the tissue is placed in fixative must be noted on the specimen requisition form.
Type of Fixative
Ten percent of NBF should be used as the fixative for breast tissue specimens as it provides optimal immunoreactivity for ER/PR; this recommendation is based on evidence from several clinically validated studies
Duration of Tissue Fixation
Breast tissue specimens must be fixed in 10 % NBF for no less than 6 h and for not more than 72 h before processing. Formalin penetrates tissue at a rate of approximately 1 mm/h; the chemical reaction of fixation, which involves protein cross-linking by formaldehyde, begins after formaldehyde has penetrated into the tissue and is time dependant. Underfixation or overfixation of breast tissue may lead to false-negative ER results.
Analytic Standardization
Antibody selection for ER testing.
Antibodies used for ER/PR testing should have well-documented specificity and sensitivity and should have been clinically validated.
Analytic Standardization
Positive and negative batch controls, with defined high positive, negative, and intermediate levels of receptor content should be included with every ER and PR IHC assay batch run. Batch controls are useful in monitoring assay performance and will detect loss of sensitivity or assay analytic drift. On-slide external controls and internal normal epithelial elements should also be assessed to ensure that the assay is performing properly.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


