(1)
Chennai Breast Centre, Chennai, India
Knowledge of normal sonographic anatomy of the breast and ultrasound criteria that differentiate or overlap between the benign and malignant breast masses is one of the most important operator- or examiner-dependent factors in breast ultrasound.
Use of consistent terminology and clear communication of the ultrasound findings are critical in patient management. Many of the descriptors have been validated in several studies, and ACR has developed a lexicon for findings seen by ultrasound. This includes terminology to describe the shape, orientation, margins, echogenicity, homogeneity, posterior acoustic features, boundary zone, and effect on surrounding tissues on the breast lesions/masses.
The internal heterogeneity of breast cancers accounts for multiple findings being present partially, completely, or sometimes even absent. Complete scanning of lesion in two orthogonal planes ensures that no finding is missed.
Shape of Lesion
Ovoid masses with less than three gentle lobulations, in general, are benign, whereas a round shape is not reassuring. A well-differentiated malignancy can appear round, and benign lesions like cysts can also be round. Round complex cysts can be quite challenging to differentiate from a solid lesion (Figs. 12.1, 12.2, and 12.3).
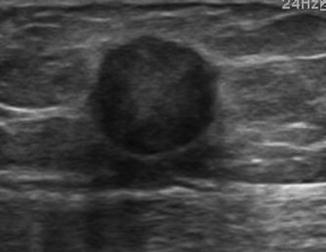
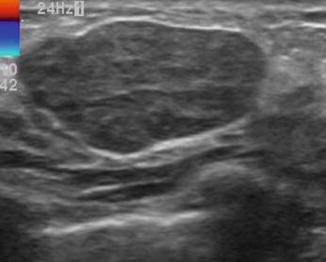
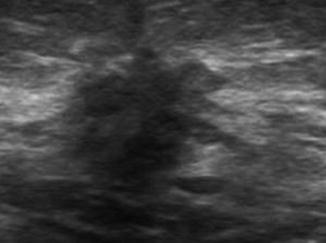
Fig. 12.1
Rounded lesion
Fig. 12.2
Oval lesion
Fig. 12.3
Irregular lesion
Margins
The lesion should always be scanned in two orthogonal planes for definition of its margin.
Circumscribed Margin
The presence of a well-circumscribed lesion with complete, thin echogenic capsule is indicative of a benign lesion. The echogenic capsule should be demonstrated in its entirety as it is sometimes difficult to see the capsule around the edges of a lesion due to critical angle effect. Heeling and toeing of the probe will demonstrate the completeness of the capsule. Well-differentiated malignancies can also have circumscribed margins, but it may not have complete capsule and they are less likely to be elliptical and or gently lobulated. The combined presence of elliptical or gently lobulated lesion with a complete capsule is indicative of a benign lesion (Fig. 12.4).
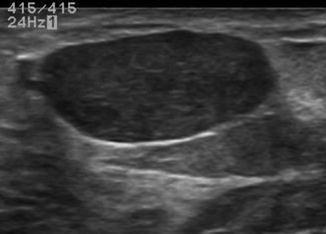
Fig. 12.4
Lesion with circumscribed margin
Angular Margin
The presence of an angular margin is highly suspicious for a malignancy (Fig. 12.5).
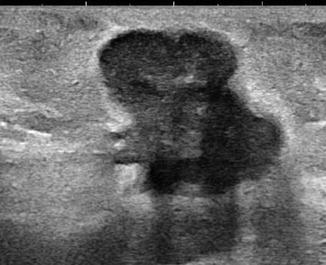
Fig. 12.5
Lesion showing angular margins
Microlobulated Margin
Microlobulations are small, 1–2-mm lobulations that occur in the periphery of the mass. They may be seen along the entire lesion or in parts. Both invasive and in situ cancers can have microlobulated margins (Fig. 12.6).
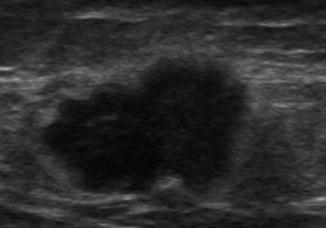
Fig. 12.6
Lesion with micro lobulated margins
Spiculated Margin
Spiculated margin is characteristic of malignant lesions. Spiculations tend to be seen along the lateral edges of the lesion as the spicules are perpendicular to the ultrasound beam. They are less well seen anteriorly and posteriorly because they are parallel to the ultrasound beam. Besides, the posterior acoustic shadowing might also obscure the spiculations (Fig. 12.7).
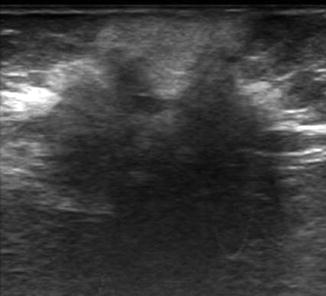
Fig. 12.7
Lesion with spiculated margins
Boundary Zone
An abrupt transition zone between the lesion and the normal tissue is usually benign. An echogenic halo around the lesion is suggestive of malignancy. The thick echogenic halo is usually due to a peritumoral edema or spicules that are too small to be resolved sonographically (Fig. 12.8).
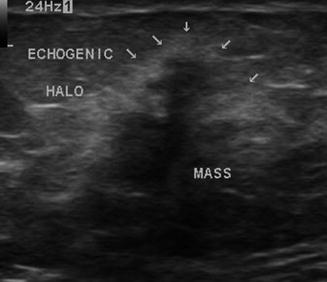
Fig. 12.8
Taller than wide irregular hypoechoic lesion with surrounding echogenic halo in a case of invasive ductal carcinoma. The echogenic halo is more prominent along the lateral aspect of the lesion
Axial Orientation
The axial orientation of mass in relation to the chest wall should be assessed. Benign lesions grow parallel to the tissue planes and remain within the tissue planes. The long axis of benign lesions are transverse, i.e., “wider than taller” in appearance. Malignant lesions invade and grow against the tissue planes and the long axis is likely to be vertical, i.e., “taller than wider” in appearance (Figs. 12.9 and 12.10).
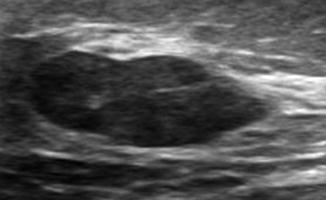
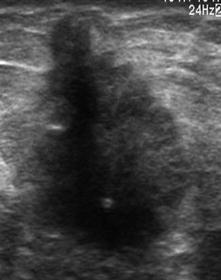
Fig. 12.9
Benign lesion: wider than tall hypoechoic lesion
Fig. 12.10
Malignant lesion: taller than wide hypoechoic lesion with irregular margins
Echogenicity
The echogenicity of breast lesions should be compared with the echogenicity of fat in the breast. Ultrasound settings should be adjusted such that fat appears medium gray. Gain settings are very important in assessing the echogenicity of the lesion. Incorrect gain settings can make a cyst appear solid and a solid lesion appear like a cyst.
Intensely hyperechoic lesions are benign. They are brighter appearing than the fat (Fig. 12.11).
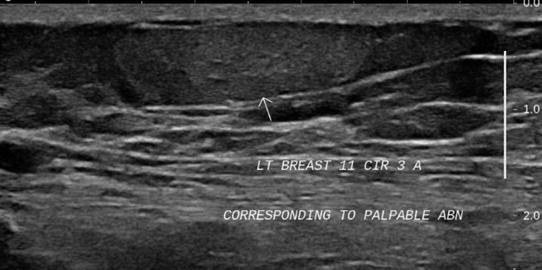
Fig. 12.11
Hyperechoic lesion in the premammary zone suggestive of lipoma
Isoechoic lesions have an echogenicity similar to that of fat. Lipomas and few fibroadenomas can appear isoechoic (Fig. 12.12). Some malignant lesions can also be isoechoic. Vocal fremitus with power Doppler may help to distinguish an isoechoic abnormal area from normal isoechoic tissue.
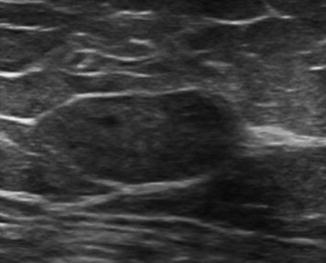
Fig. 12.12
Ovoid isoechoic lesion
Hypoechoic lesions are those that are darker than the fat. Fibroadenomas, complex echogenic cysts, and most carcinomas are hypoechoic (Fig. 12.13). With newer high-end machines, the frequency, bandwidth, and dynamic range have all been increased, which offsets the contrast resolution. This sometimes makes hypoechoic lesions appear isoechoic or mildly hypoechoic.
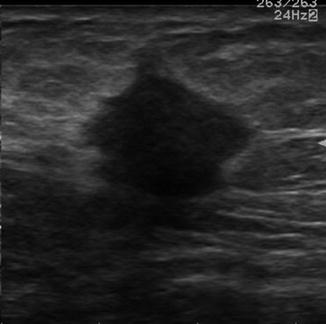
Fig. 12.13




Hypoechoic nonparallel lesion with angular and spiculated margins
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
