Fig. 43.1.
T12–L1 thoracolumbar nerve root compression with referred pain.
Physical Examination
Physical exam begins with examination of the spine with the patient in a prone position. Lateral pressure on the spinous processes of T9–L3 should elicit unilateral pain. The compression should be performed in both a right and left movement. Direct compression over the affected facet will elicit the same tenderness (Fig. 43.2). The posterior iliac crest should then be palpated to identify point tenderness. Rubbing the crest in an up-and-down motion should elicit pain at a point usually 7 cm from the midline. The pain should be sharp in nature. This point is called the posterior iliac crest point; it is where the irritated cutaneous branches of T11–L1 are compressed [3] (Fig. 43.3).
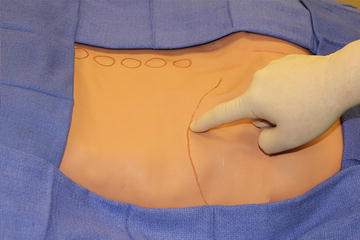
Fig. 43.2.
Point pressure over iliac crest.
Fig. 43.3.
Anatomical position of the L1–L3 as it transverses the iliac crest.
The pinch–roll test is then performed to test for hyperalgesia of the skin and subcutaneous tissues of the gluteal and iliac crest region. Referred pain accompanies hyperalgesia and thickening of the skin. The test is performed by grasping a fold of skin between the thumb and forefinger and rolling the tissue in a controlled manner. The involved side should elicit tenderness compared to the opposite side [4] (Fig. 43.4).

Fig. 43.4.
Pinch–roll test.
Groin pain should be examined with standard inguinal examination to rule out inguinal hernia. Thoracolumbar syndrome has two clinical features that are characteristic: a positive pinch–roll test and tenderness on the superior aspect of the pubis. Palpation of the periosteum of the pubis should cause tenderness on the affected side. The pinch–roll test should be performed in a supine position in the inguinal area [2].
Related posts:
 Introduction to Primary and Secondary Groin Pain: What Is Inguinodynia?
Prevention of Pain: Optimizing the Laparoscopic TEP and TAPP Techniques
Prophylactic Neurectomy Versus Pragmatic Neurectomy
Patient with Referred Hip Pain
Introduction to Primary and Secondary Groin Pain: What Is Inguinodynia?
Prevention of Pain: Optimizing the Laparoscopic TEP and TAPP Techniques
Prophylactic Neurectomy Versus Pragmatic Neurectomy
Patient with Referred Hip Pain
 Chronic Pelvic Pain in Women
Chronic Pelvic Pain in Women
 Groin Pain Etiology: Hip-Referred Groin Pain
Groin Pain Etiology: Hip-Referred Groin Pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


