Chapter 24 Surgical diathermy
Physical principles
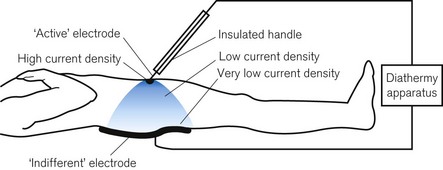
Radio frequency (RF) surgical diathermy or electrosurgery uses the heat generated by an electric current,1 often delivered at more than 200 V, passing through a small amount of tissue to cut, destroy or vaporize that tissue and to create haemostasis by causing coagulation and sealing of small blood vessels. Passing an electric current through the body causes all the tissue through which it passes to heat up. For this effect to be clinically useful, the current must pass through a small area of tissue at the active electrode. In contrast, at the indifferent electrode of the diathermy plate, which completes the electrical circuit, the current must pass from the skin surface to a large area to prevent burns where they are undesirable. This is the concept of current density.
Current density
Current density refers to the current per unit cross-sectional area. With a large conductive area, such as at the patient plate, there is a low current density and, although the amount of heat generated is the same at the active electrode, the heat is rapidly conducted away. At the contact point of the active electrode, the current density is high, the heat being generated over a small area, thus creating the desired surgical effect (Fig. 24.1).
It is necessary to pass considerable currents through the human body to produce enough heat to have this effect. Under normal circumstances, the accidental passage of electric current at mains frequency (50 Hz) through the body has several highly undesirable effects, including burns, muscle spasm leading to asphyxiation and ventricular fibrillation. However, it was found experimentally years ago that, although living tissues, especially conducting and contractile tissues, are maximally sensitive to electric current at mains frequency, this sensitivity decreases at lower frequencies (including direct current (DC)) and decreases markedly at very high frequencies (Fig. 23.3).
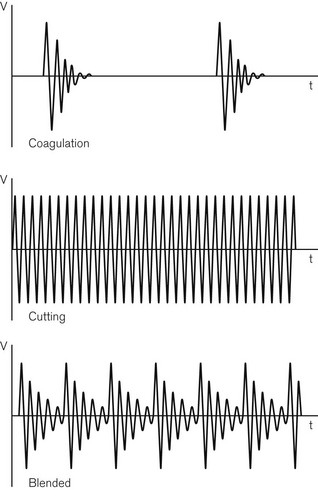
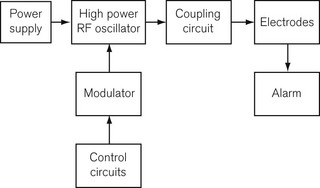
Diathermy frequencies used in surgery are in the region of 0.4–1.5 MHz. RF diathermy machines are, in fact, powerful radio transmitters and would cause severe interference to radio receivers, even at some distance. Without good screening, RF diathermy signals can capacitatively couple with ECG or other amplifiers and grossly interfere with the biological signal being monitored. For this reason, by international agreement, only certain narrow frequency bands are used. A sine waveform has been found to be better for cutting and a damped waveform for coagulation (Fig. 24.2). A combined waveform is also available, usually referred to as ‘blend’, which is commonly used during cystoscopic resections of a bladder tumour or prostate. Although the frequency band is narrow, the current required to produce an effect may vary widely between patients as shown in a study in patients during prostatectomy.2 A block diagram of a RF diathermy machine is shown in Fig. 24.3. A high-power, high-frequency oscillator or generator is controlled by a modulator to produce the necessary waveforms. The output of the generator is led through coupling circuits to optimize impedance matching between the generator and the ‘indifferent’ and the ‘active’ electrodes. The circuitry normally contains a 0.01 µF capacitor from the indifferent electrode to earth. It will be recalled that the electrical impedance (the term used to describe electrical resistance at different frequencies of current) is inversely proportional to both the frequency of the current and the magnitude of the capacitance; therefore, this capacitor in the diathermy circuit provides a low impedance (20 Ω) route to earth for the high-frequency diathermy current, but a high impedance (300 kΩ) to any incidental low-frequency mains current. This effectively isolates the circuit from earth against mains leakage current. The risk of electrocution from a diathermy apparatus is, therefore, much reduced, but the risk of burns should not be underestimated (see below). Where the indifferent lead (i.e. the plate) socket is at earth potential, as it is in many older diathermy sets, it is vitally important that the lead is connected to the correct terminal of the diathermy apparatus. If the plate were accidentally connected to the active terminal, when the foot switch is depressed the patient might be burned at all points connected to earth (i.e. where the body is in contact with those parts of the operating table at earth potential).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


