![]() Emergency venous access for fluid resuscitation and drug infusion
Emergency venous access for fluid resuscitation and drug infusion
![]() Central venous pressure and oxygen monitoring
Central venous pressure and oxygen monitoring
![]() Infusions requiring central venous administration (vasopressors, hyperosmolar solutions, hyperalimentation)
Infusions requiring central venous administration (vasopressors, hyperosmolar solutions, hyperalimentation)
![]() Routine venous access due to inadequate peripheral IV sites
Routine venous access due to inadequate peripheral IV sites
![]() Introduction of pulmonary artery catheter
Introduction of pulmonary artery catheter
![]() Introduction of transvenous pacing wire
Introduction of transvenous pacing wire
CONTRAINDICATIONS
![]() No absolute contraindications
No absolute contraindications
![]() Relative Contraindications
Relative Contraindications
![]() Coagulopathic patients (inability to compress)
Coagulopathic patients (inability to compress)
![]() Overlying infection, burn, or skin damage at puncture site
Overlying infection, burn, or skin damage at puncture site
![]() Distorted anatomy or trauma at the cannulation site
Distorted anatomy or trauma at the cannulation site
![]() Combative or uncooperative patients
Combative or uncooperative patients
![]() Penetrating trauma with suspected proximal vascular injury
Penetrating trauma with suspected proximal vascular injury
![]() Pneumothorax on contralateral side (risk of bilateral pneumothoraces)
Pneumothorax on contralateral side (risk of bilateral pneumothoraces)
![]() Chronic obstructive pulmonary disease (COPD)
Chronic obstructive pulmonary disease (COPD)
RISKS/CONSENT ISSUES
![]() Pain
Pain
![]() Local bleeding and hematoma
Local bleeding and hematoma
![]() Infection
Infection
![]() Pneumothorax/hemothorax (necessitating chest tube)
Pneumothorax/hemothorax (necessitating chest tube)
![]() General Basic Steps
General Basic Steps
![]() Analgesia
Analgesia
![]() Insertion
Insertion
![]() Seldinger technique
Seldinger technique
![]() Dilation
Dilation
![]() Catheter insertion
Catheter insertion
![]() Confirmation
Confirmation
![]() Flush and secure
Flush and secure
LANDMARKS
Right subclavian vein (SCV) approach is preferred because (1) pleural dome is lower on the right and (2) thoracic duct is on the left.
![]() Infraclavicular Approach (FIGURE 24.1)
Infraclavicular Approach (FIGURE 24.1)
![]() Place the left index finger on the suprasternal notch and the thumb on the costoclavicular junction
Place the left index finger on the suprasternal notch and the thumb on the costoclavicular junction
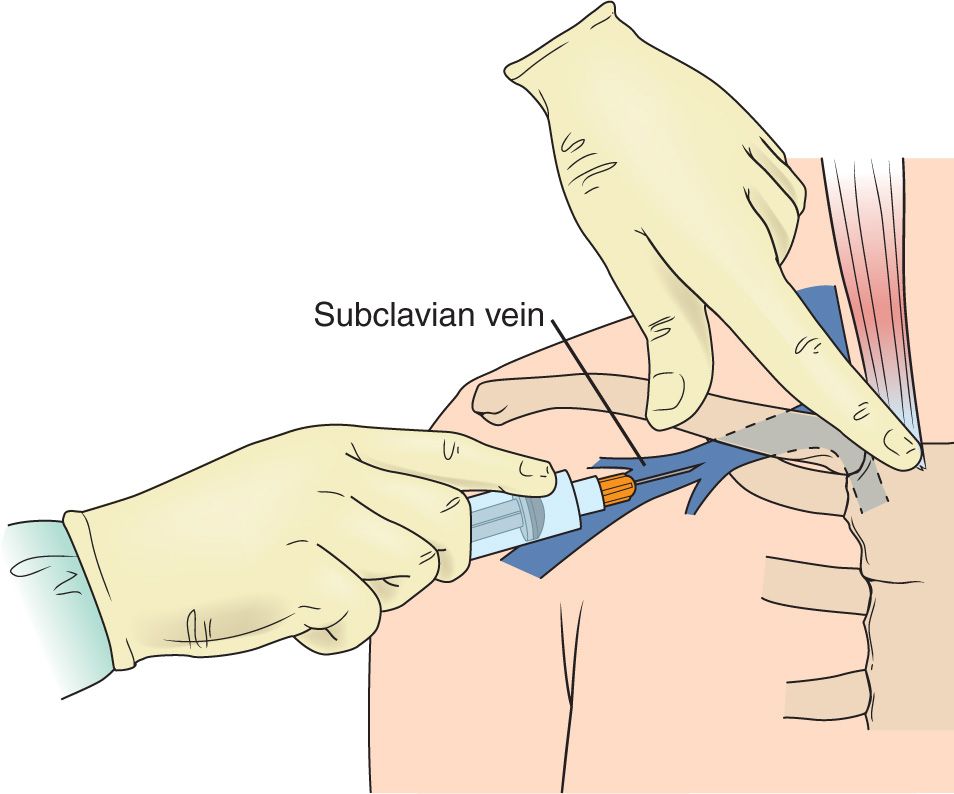
FIGURE 24.1 Infraclavicular approach to subclavian vein cannulation. Needle insertion at the bisection of the medial and middle thirds of the clavicle. Aim the needle toward the suprasternal notch.
![]() Needle insertion is at the bisection of the medial and middle thirds of the clavicle
Needle insertion is at the bisection of the medial and middle thirds of the clavicle
![]() Aim the needle toward suprasternal notch
Aim the needle toward suprasternal notch
![]() Needle bevel is oriented inferomedially to facilitate wire entry
Needle bevel is oriented inferomedially to facilitate wire entry
![]() Supraclavicular Approach (FIGURE 24.2)
Supraclavicular Approach (FIGURE 24.2)
![]() Needle insertion is just above the clavicle, 1 cm lateral to the insertion of clavicular head of sternocleidomastoid (SCM)
Needle insertion is just above the clavicle, 1 cm lateral to the insertion of clavicular head of sternocleidomastoid (SCM)
![]() Aim to bisect angle between SCM and clavicle with the needle tip pointing toward the contralateral nipple
Aim to bisect angle between SCM and clavicle with the needle tip pointing toward the contralateral nipple
![]() Needle bevel is oriented medially
Needle bevel is oriented medially
SUPPLIES
![]() Central Venous Catheter Kit
Central Venous Catheter Kit
![]() Drapes, chlorhexidine prep (2), gauze
Drapes, chlorhexidine prep (2), gauze
![]() Catheter (multiport, cordis, or hemodialysis)
Catheter (multiport, cordis, or hemodialysis)
![]() Guidewire within plastic sheath
Guidewire within plastic sheath
![]() Lidocaine, anesthesia syringe, and small-gauge needle
Lidocaine, anesthesia syringe, and small-gauge needle
![]() Three-inch introducer needle and syringe
Three-inch introducer needle and syringe
![]() Dilator
Dilator
![]() Scalpel
Scalpel
![]() Suture
Suture
![]() Sterile gloves, sterile gown, sterile cap and mask
Sterile gloves, sterile gown, sterile cap and mask
![]() Sterile drapes
Sterile drapes
![]() Sterile saline flushes
Sterile saline flushes
![]() Sterile port caps
Sterile port caps
![]() Ultrasound machine (optional)
Ultrasound machine (optional)
![]() Sterile ultrasound probe cover with sterile gel (optional)
Sterile ultrasound probe cover with sterile gel (optional)
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Cardiac monitoring to detect dysrhythmias triggered by the wire being advanced into the right ventricle
Cardiac monitoring to detect dysrhythmias triggered by the wire being advanced into the right ventricle
![]() Supplemental oxygen and continuous pulse oximetry monitoring
Supplemental oxygen and continuous pulse oximetry monitoring
![]() Lower the head of the bed to 15 to 30 degrees in Trendelenburg position
Lower the head of the bed to 15 to 30 degrees in Trendelenburg position
![]() Place a rolled up towel or sheet in between the patient’s shoulder blades to elevate the patient’s clavicle and provide better access to the SCV (optional)
Place a rolled up towel or sheet in between the patient’s shoulder blades to elevate the patient’s clavicle and provide better access to the SCV (optional)
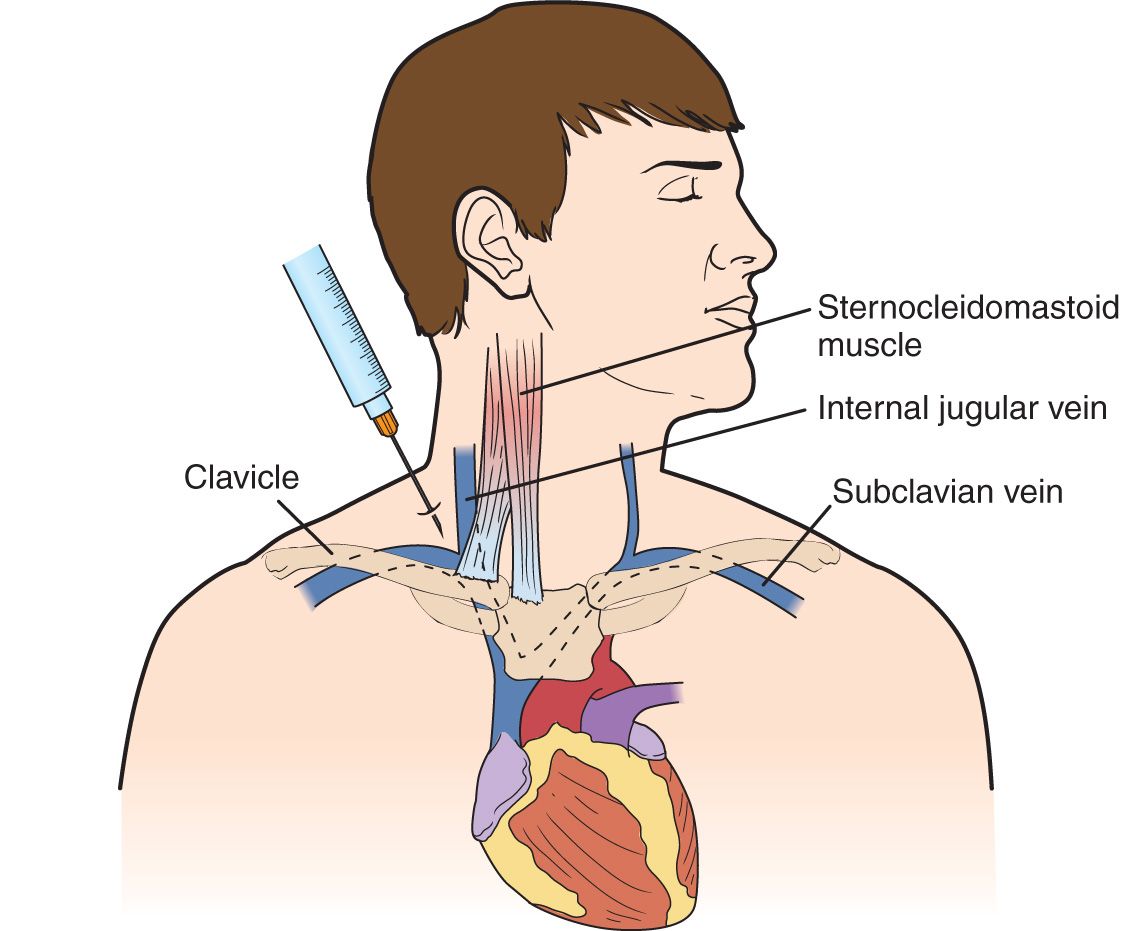
FIGURE 24.2 Supraclavicular approach to subclavian vein cannulation. Needle insertion is just above the clavicle, 1 cm lateral to the insertion of clavicular head of sternocleidomastoid (SCM). Aim to bisect angle between SCM and clavicle with the needle tip pointing toward the contralateral nipple. The needle tip is pointed 10 degrees above horizontal.
![]() Place the ipsilateral arm in abduction
Place the ipsilateral arm in abduction
![]() Sterilize clavicular insertion site, including ipsilateral neck in case subclavian vascular access fails and internal jugular (IJ) vascular access is necessary
Sterilize clavicular insertion site, including ipsilateral neck in case subclavian vascular access fails and internal jugular (IJ) vascular access is necessary
![]() Wear surgical cap, eye protection, mask, sterile gown and gloves
Wear surgical cap, eye protection, mask, sterile gown and gloves
![]() Drape with sterile sheets to cover the patient’s head and legs
Drape with sterile sheets to cover the patient’s head and legs
Note: Unless immediate emergent access is necessary, the procedure must be performed in full sterile technique (i.e., cap, eye protection, mask, sterile gown, and sterile gloves).
![]() Analgesia
Analgesia
![]() Use a small-bore needle (25 gauge) to anesthetize the skin and subcutaneous tissue with 1% lidocaine
Use a small-bore needle (25 gauge) to anesthetize the skin and subcutaneous tissue with 1% lidocaine
![]() Insertion
Insertion
![]() Infraclavicular Approach
Infraclavicular Approach
![]() Place the left index finger on the suprasternal notch and the thumb on the costoclavicular junction
Place the left index finger on the suprasternal notch and the thumb on the costoclavicular junction
![]() The needle insertion is at the bisection of medial and middle thirds of the clavicle
The needle insertion is at the bisection of medial and middle thirds of the clavicle
![]() Aim the needle toward the suprasternal notch with the bevel oriented inferomedially
Aim the needle toward the suprasternal notch with the bevel oriented inferomedially
![]() At a shallow angle to the skin, advance the needle just posterior to the clavicle at the junction of middle and medial thirds
At a shallow angle to the skin, advance the needle just posterior to the clavicle at the junction of middle and medial thirds
![]() Apply posterior pressure on the needle to direct it under the clavicle, aiming toward suprasternal notch
Apply posterior pressure on the needle to direct it under the clavicle, aiming toward suprasternal notch
![]() The needle should be parallel to the bed as it is advanced. Avoid advancing the needle posteriorly into the dome of the lung.
The needle should be parallel to the bed as it is advanced. Avoid advancing the needle posteriorly into the dome of the lung.
![]() Aspirate continuously while advancing the needle
Aspirate continuously while advancing the needle
![]() If redirecting the needle, always withdraw the needle to the level of skin first
If redirecting the needle, always withdraw the needle to the level of skin first
![]() Once the vessel is located, free-flowing venous blood is aspirated
Once the vessel is located, free-flowing venous blood is aspirated
![]() Stabilize and hold the introducer needle in place with the nondominant hand
Stabilize and hold the introducer needle in place with the nondominant hand
![]() Gently remove the syringe from the needle and occlude the hub with your thumb to minimize the risk of air embolism
Gently remove the syringe from the needle and occlude the hub with your thumb to minimize the risk of air embolism
![]() Supraclavicular Approach
Supraclavicular Approach
![]() The needle insertion is just above the clavicle, 1 cm lateral to the insertion of clavicular head of SCM
The needle insertion is just above the clavicle, 1 cm lateral to the insertion of clavicular head of SCM
![]() Aim to bisect the angle between SCM and clavicle with the tip pointing just caudal to the contralateral nipple
Aim to bisect the angle between SCM and clavicle with the tip pointing just caudal to the contralateral nipple
![]() Direct the needle 10 to 15 degrees upward from the horizontal plane, just posterior to the clavicle, again aiming just caudal to the contralateral nipple
Direct the needle 10 to 15 degrees upward from the horizontal plane, just posterior to the clavicle, again aiming just caudal to the contralateral nipple
![]() The needle bevel is oriented medially
The needle bevel is oriented medially
![]() Note that the SCV is found more superficially in the supraclavicular approach than in the infraclavicular approach
Note that the SCV is found more superficially in the supraclavicular approach than in the infraclavicular approach
![]() Aspirate continuously while advancing the needle
Aspirate continuously while advancing the needle
![]() If redirecting the needle, always withdraw the needle to the level of skin first
If redirecting the needle, always withdraw the needle to the level of skin first
![]() Once the vessel is located, free-flowing venous blood is aspirated. Successful puncture usually occurs at a depth of 2 to 3 cm.
Once the vessel is located, free-flowing venous blood is aspirated. Successful puncture usually occurs at a depth of 2 to 3 cm.
![]() Stabilize and hold the introducer needle in place with the nondominant hand
Stabilize and hold the introducer needle in place with the nondominant hand
![]() Gently remove the syringe from the needle and occlude the hub with your thumb to minimize the risk of air embolism
Gently remove the syringe from the needle and occlude the hub with your thumb to minimize the risk of air embolism
![]() Seldinger Technique
Seldinger Technique
![]() Advance the guidewire through the introducer needle. The wire should pass easily. Do not force the guidewire.
Advance the guidewire through the introducer needle. The wire should pass easily. Do not force the guidewire.
![]() Always hold on to the guidewire with one hand. Never let go of the guidewire.
Always hold on to the guidewire with one hand. Never let go of the guidewire.
![]() If resistance is met, withdraw the wire and rotate it, adjust the angle of needle entry, or remove the wire and reaspirate with the syringe to ensure the needle is still in the vessel
If resistance is met, withdraw the wire and rotate it, adjust the angle of needle entry, or remove the wire and reaspirate with the syringe to ensure the needle is still in the vessel
![]() When at least half of the guidewire is advanced, remove the needle over the wire. Keep one hand holding the wire at all times.
When at least half of the guidewire is advanced, remove the needle over the wire. Keep one hand holding the wire at all times.
![]() Make a superficial skin incision with the bevel of the scalpel blade angled away from wire
Make a superficial skin incision with the bevel of the scalpel blade angled away from wire
![]() Ensure the incision is large enough to allow easy passage of the dilator
Ensure the incision is large enough to allow easy passage of the dilator
![]() Dilation
Dilation
![]() Thread the dilator over the guidewire, always holding on to the wire
Thread the dilator over the guidewire, always holding on to the wire
![]() Advance the dilator through the skin into the vessel with a firm, twisting motion while holding the guidewire with the nondominant hand
Advance the dilator through the skin into the vessel with a firm, twisting motion while holding the guidewire with the nondominant hand
![]() Remove the dilator, leaving the guidewire in place
Remove the dilator, leaving the guidewire in place
![]() Catheter Insertion
Catheter Insertion
![]() Thread the catheter over the wire and retract the wire until it emerges from the catheter’s port
Thread the catheter over the wire and retract the wire until it emerges from the catheter’s port
![]() While holding the guidewire, advance the catheter through the skin into the vessel to the desired depth. Optimal depth depends on patient size and is typically 10 to 15 cm for the right SCV and 14 to 19 cm for the left SCV.
While holding the guidewire, advance the catheter through the skin into the vessel to the desired depth. Optimal depth depends on patient size and is typically 10 to 15 cm for the right SCV and 14 to 19 cm for the left SCV.
![]() Withdraw the guidewire through the catheter
Withdraw the guidewire through the catheter
![]() Use a syringe to aspirate blood from the catheter to confirm placement in the vein
Use a syringe to aspirate blood from the catheter to confirm placement in the vein
![]() Confirmation
Confirmation
![]() Manometry
Manometry
![]() Blood gas analysis
Blood gas analysis
![]() Sonographic confirmation of the catheter in the vein
Sonographic confirmation of the catheter in the vein
![]() Post procedure chest x-ray (CXR)
Post procedure chest x-ray (CXR)
![]() Confirm the catheter tip is in the superior vena cava just proximal to the right atrium
Confirm the catheter tip is in the superior vena cava just proximal to the right atrium
![]() Rule out pneumothorax
Rule out pneumothorax
![]() Flush and Secure
Flush and Secure
![]() Aspirate, flush, and heplock all central line lumens
Aspirate, flush, and heplock all central line lumens
![]() Suture the catheter to the skin by using silk or nylon sutures
Suture the catheter to the skin by using silk or nylon sutures
![]() Cover the skin insertion site with sterile dressing (bacteriostatic if available)
Cover the skin insertion site with sterile dressing (bacteriostatic if available)
COMPLICATIONS
![]() Dysrhythmias
Dysrhythmias
![]() Arterial puncture or cannulation
Arterial puncture or cannulation
![]() Vessel laceration or dissection
Vessel laceration or dissection
![]() Pneumothorax or hemothorax
Pneumothorax or hemothorax
![]() Brachial plexus injury
Brachial plexus injury
![]() Phrenic nerve injury
Phrenic nerve injury
![]() Tracheal puncture or endotracheal cuff perforation
Tracheal puncture or endotracheal cuff perforation
![]() Guidewire embolism
Guidewire embolism
![]() Air embolism
Air embolism
![]() Catheter tip embolism
Catheter tip embolism
![]() Catheter malposition
Catheter malposition
![]() Venous thrombosis
Venous thrombosis
![]() Insertion site cellulitis
Insertion site cellulitis
![]() Line sepsis
Line sepsis
![]() Local hematoma
Local hematoma
ULTRASOUND-GUIDED CENTRAL VENOUS ACCESS
![]() Use of ultrasound guidance to place IJ and femoral central venous catheters has been shown to increase success rates and decrease complications
Use of ultrasound guidance to place IJ and femoral central venous catheters has been shown to increase success rates and decrease complications
![]() Current literature suggests that the use of ultrasound guidance can be helpful when placing subclavian central venous catheters
Current literature suggests that the use of ultrasound guidance can be helpful when placing subclavian central venous catheters
SONOGRAPHIC TECHNIQUE
![]() Place a high-frequency linear probe (5–10 MHz) just inferior to the middle and medial thirds of the clavicle with the probe marker pointed cephalad (a probe with a smaller footprint will allow better visualization of the subclavian anatomy)
Place a high-frequency linear probe (5–10 MHz) just inferior to the middle and medial thirds of the clavicle with the probe marker pointed cephalad (a probe with a smaller footprint will allow better visualization of the subclavian anatomy)
![]() Obtain a transverse view of SCV inferior to the clavicle and superior to the 1st rib. Use color flow and/or Doppler to distinguish the artery from vein (FIGURE 24.3).
Obtain a transverse view of SCV inferior to the clavicle and superior to the 1st rib. Use color flow and/or Doppler to distinguish the artery from vein (FIGURE 24.3).
![]() Rotate the probe 90 degrees, visualizing the vein continuously, and obtain a longitudinal view of SCV. Because of the clavicle, the probe may need to be moved laterally to visualize the SCV as it becomes the axillary vein distal to the 1st rib.
Rotate the probe 90 degrees, visualizing the vein continuously, and obtain a longitudinal view of SCV. Because of the clavicle, the probe may need to be moved laterally to visualize the SCV as it becomes the axillary vein distal to the 1st rib.
![]() Use color flow and/or Doppler to distinguish the vein from artery (FIGURE 24.4)
Use color flow and/or Doppler to distinguish the vein from artery (FIGURE 24.4)
![]() Maintain a longitudinal view of the SCV (stabilize the hand holding the probe on the patient’s chest to keep the probe in position)
Maintain a longitudinal view of the SCV (stabilize the hand holding the probe on the patient’s chest to keep the probe in position)
![]() Insert the introducer needle at a 30- to 45-degree angle to the skin in line with the long axis of the ultrasound probe
Insert the introducer needle at a 30- to 45-degree angle to the skin in line with the long axis of the ultrasound probe
![]() Note that the probe marker is facing the needle entry site and the needle should enter the skin directly next to the probe (FIGURE 24.5)
Note that the probe marker is facing the needle entry site and the needle should enter the skin directly next to the probe (FIGURE 24.5)
![]() The needle must be parallel to the long axis of the ultrasound probe to be visualized
The needle must be parallel to the long axis of the ultrasound probe to be visualized
![]() This in-plane approach allows direct visualization of the entire needle shaft and tip as it enters the vein and decreases the risk of pneumothorax and arterial puncture
This in-plane approach allows direct visualization of the entire needle shaft and tip as it enters the vein and decreases the risk of pneumothorax and arterial puncture
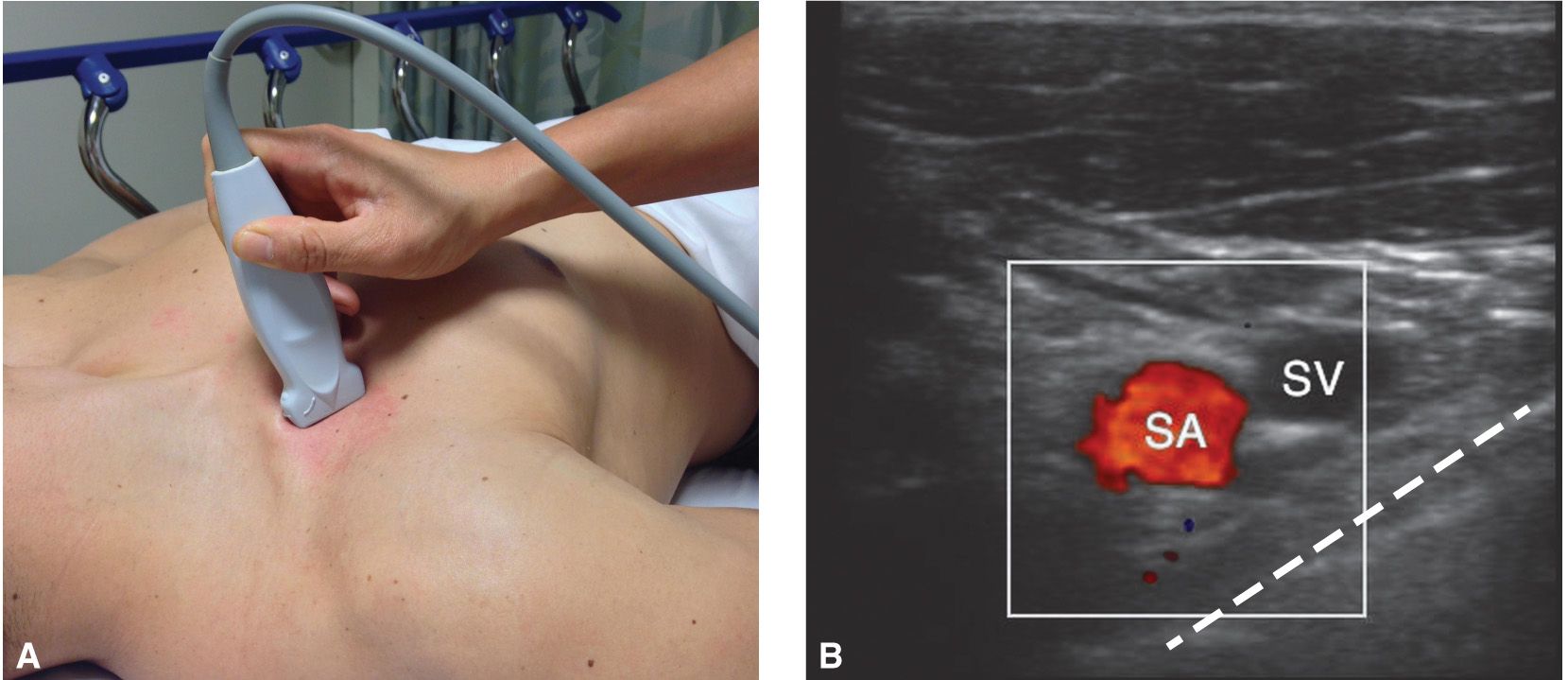
FIGURE 24.3 A: Ultrasound probe inferior to the clavicle with probe marker pointed cephalad. B: Subclavian artery (SA, red) and subclavian vein (SCV) with color flow just superior to the 1st rib and pleural line (dashed line).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


