Chapter 35 Structure and Development of the Upper Respiratory System in Infants and Children
Developmental Anatomy of the Upper Airway
The embryogenesis of the larynx is complex. The cartilages and muscles are derived from the fourth and sixth branchial arches, and the epithelium is derived from the endoderm of the laryngotracheal tube. As this epithelium rapidly proliferates, the larynx is temporarily occluded until the 10th week, when recanalization occurs. Failure to recanalize can result in laryngeal webs, stenosis, or, rarely, atresia. The epiglottis forms by mesenchymal proliferation of the third and fourth branchial arches (Figure 35-1).
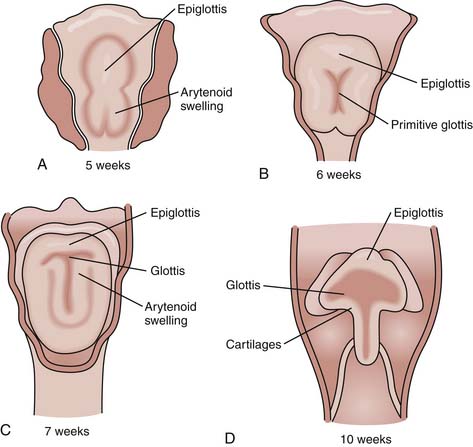
Figure 35–1 The embryologic development of the larynx.
(Modified from Arvedson J, Brodsky L: Pediatric feeding and swallowing: management and assessment, ed 2, Andover, United Kingdom, 2002, Thomson Learning.)
Anatomy and Physiology of the Upper Airway
Nasal Passages
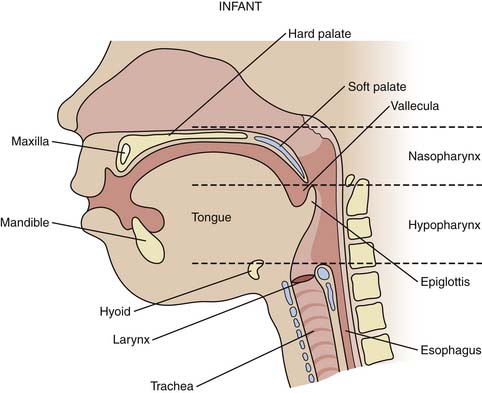
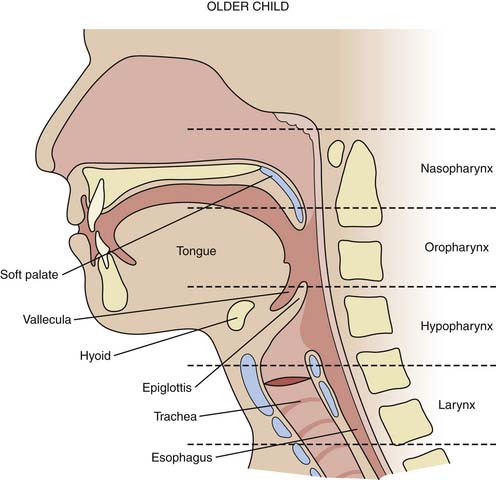
The structure of the upper airways differs in the infant (Figure 35-2), young child, and young adult (Figure 35-3). Preferential nasal breathing is present in neonates and persists up until 6 months of age due to the high riding larynx in the neck with the soft palate and vallecula in close anatomic approximation.
< div class='tao-gold-member'>





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


