75 Spine Trauma and Spinal Cord Injury
 Key Points
Key Points• Patients with spinal pain and spine fractures should receive a thorough neurologic examination to look for spinal cord injury.
• Spine fractures are associated with a high incidence of concurrent noncontiguous spine fractures and spinal cord injuries.
• The National Emergency X-radiography Utilization Study criteria or the Canadian Cervical-Spine Rule criteria can be used to identify low-risk patients who do not need cervical spine imaging.
• Imaging with plain films versus computed tomography of the cervical spine should be based on the pretest probability of a significant injury and the irradiation risk with computed tomography.
• Spinal shock, or transient physiologic transection of the spinal cord as a result of trauma, is different from neurogenic shock, which is physiologic sympathectomy of the upper spinal cord leading to peripheral vasodilation.
• Patients with a spinal cord injury caused by blunt trauma are often given high-dose corticosteroids within 8 hours of injury, although such therapy is controversial.
Epidemiology
The estimated annual cost of spine injuries, including inability to work and health care costs, exceeds $5 billion in the United States.1
In the emergency department (ED), all trauma victims are screened for vertebral fractures, ligamentous disruptions, and spinal cord injuries because of the potentially devastating neurologic consequences of overlooking these injuries. Patients with a delayed diagnosis of spinal fracture are 7.5 times more likely to sustain secondary neurologic deficits.2 Neurologic deficits from spinal cord injury may be subtle and can easily be missed if not specifically evaluated. Adding to these difficulties, plain film radiographs of the spine, though an adequate screening tool for other fractures, can miss 23% to 42% of cervical spinal fractures3,4 and 13% to 50% of lumbar fractures.5,6
Pathophysiology
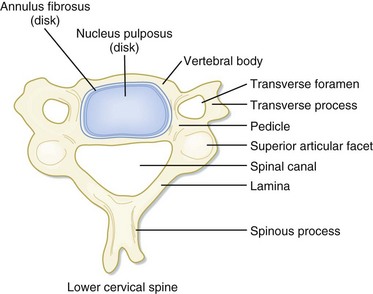
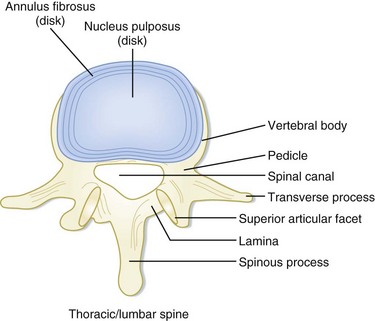
In the setting of spinal trauma, the bone, ligaments, spinal cord, and vascular structures may be injured. Anatomically, the vertebral bony spine can be divided into structural columns. The cervical spine is traditionally divided into two columns—anterior and posterior. The anterior column consists of the load-bearing vertebral bodies, intervertebral disks, anterior longitudinal ligament, and posterior longitudinal ligament (Fig. 75.1). The posterior column consists of the more posterior structures, including the pedicles, laminae, and transverse and spinous processes (Fig. 75.2).
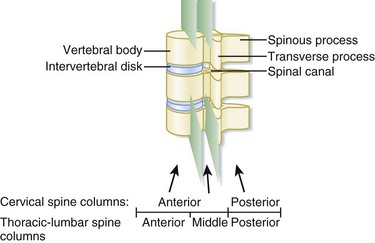
In contrast, the thoracic and lumbar vertebral spines are divided into three columns based on the modified Denis model—anterior, middle, and posterior (Fig. 75.3). The anterior column consists of the anterior longitudinal ligament, the anterior two thirds of the vertebral body, and the intervertebral disk. The middle column consists of the posterior longitudinal ligament, the posterior third of the vertebral body, and the intervertebral disk. Any disruption of the middle column predisposes a patient to significant spinal cord injury because the middle column abuts the spinal canal. The posterior column consists of the remaining posterior structures.
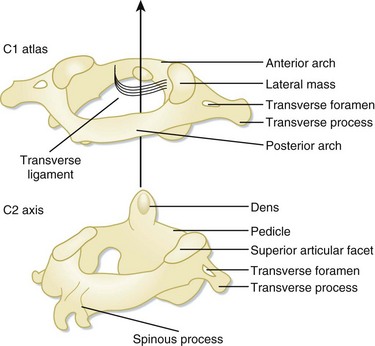
The C1 and C2 vertebrae are anatomically unique (Fig. 75.4). C1 (atlas) is a ring-link structure without a vertebral body. It articulates superiorly with the occipital condyles. This articulation allows 50% of normal neck flexion and extension. C2 (axis) projects the dens superiorly to articulate with C1. The transverse ligament tethers the dens to the anterior arch of C1. This atlantoaxial articulation allows 50% of normal neck rotation left and right.
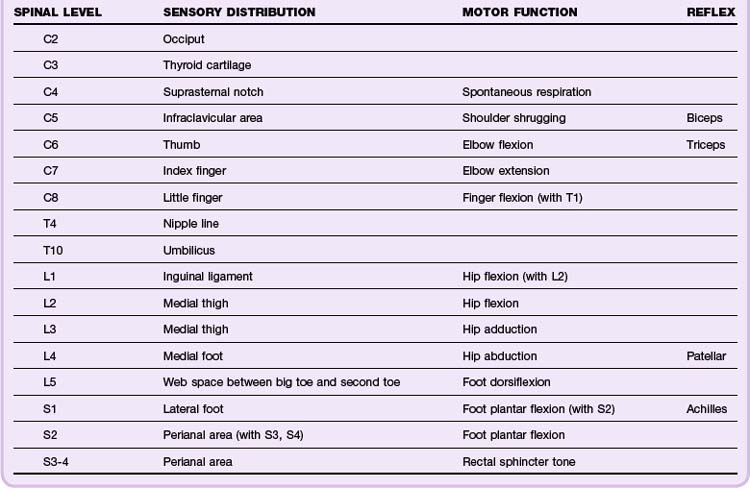
The spinal cord spans from the foramen magnum to the L1 level, whereupon the spinal cord tapers into the conus medullaris and cauda equina, a collection of peripheral lower lumbar and sacral nerve roots. Because the spinal cord is thickest in the cervical spine, there is relatively less spinal canal space in the cervical levels than in the thoracic or lumbar spine. Thus spinal cord injuries occur more frequently with cervical spine trauma than with thoracic or lumbar spine trauma. The neurologic dermatomes can help localize the injury (Table 75.1).
Presenting Signs and Symptoms
Patients with spinal cord injuries may have a spectrum of findings ranging from subtle neurologic deficits to grossly obvious paralysis. Spinal cord injuries should be suspected in any trauma victim who complains of neck or back pain, especially pain exacerbated by movement. Neurologic symptoms suggesting spinal cord injury include numbness, tingling, paresthesias, focal weakness, and paralysis. Other worrisome symptoms include urinary or fecal incontinence and urinary retention. Unconscious patients and those with impaired consciousness secondary to intoxication may harbor occult spinal cord injuries. Physical examination should focus on the spine and areas where associated injuries may occur (Tables 75.2 and 75.4).
Table 75.2 Physical Examination Findings Associated with Vertebral Fractures and Spinal Cord Injuries
| INJURY | PHYSICAL EXAMINATION AREA | ASSOCIATED FINDINGS |
|---|---|---|
| Vertebral fracture | Spine | Tenderness of the neck and/or back. Examine the entire spine because vertebral fractures may occur in multiples. |
| Neurologic | See spinal cord injury below. | |
| Chest | Thoracic spine fractures: Check for chest tenderness, unequal breath sounds, and arrhythmia, which are suggestive of an associated intrathoracic injury or myocardial contusion. | |
| Abdomen/pelvis | Thoracolumbar and lumbar spine fractures: Check for abdominal or pelvic tenderness. For instance, up to 50% of patients with a transverse process fracture7 and 33% of patients with a Chance fracture8 have concurrent intraabdominal pathology. A transverse area of ecchymosis on the lower abdominal wall (seat belt sign) increases the chance of an abdominopelvic injury. | |
| Extremity | Thoracolumbar and lumbar spine fractures: Check for calcaneal tenderness because 10% of calcaneal fractures are associated with a low thoracic or lumbar fracture. Mechanistically, these areas are fractured as a result of axial loading. | |
| Spinal cord injury | Neurologic, motor (anterior column) | Assess motor function on a scale of 0 to 5 (see Table 75.3). motor level is defined as the most caudal segment with at least 3/5 strength. Injuries to the first eight cervical segments result in tetraplegia (previously known as quadriplegia); lesions below the T1 level result in paraplegia. |
| Neurologic, sensory (spinothalamic tract) | Assess sensory function via pinprick and light touch on the following scale: 0 = absent; 1 = impaired; 2 = normal. The sensory level is defined as the most caudal segment of the spinal cord with normal sensory function. The highest intact sensory level should be marked on the patient’s spine to monitor for progression. | |
| Neurologic, sensory (dorsal column) | Assess vibratory sensory function on a scale of 0 to 2 by using a tuning fork over bony prominences. Assess position sense (proprioception) by flexing and extending the great toe. | |
| Neurology, deep tendon reflex | On a scale of 0 to 4, assess the deep tendon reflexes in the upper (biceps, triceps) and lower (patellar, Achilles) extremities (see Table 75.4). | |
| Anogenital | Assess rectal tone, sacral sensation, signs of urinary or fecal retention or incontinence, and priapism. Also check the anogenital reflexes: an anal wink (S2-S4) is present if the anal sphincter contracts in response to stroking the perianal skin area. The bulbocavernosus reflex (S3-S4) is elicited by squeezing the glans penis or clitoris (or pulling on an inserted Foley catheter), which results in reflexive contraction of the anal sphincter. | |
| Head-to-toe examination | A spinal cord injury may mask a patient’s ability to perceive and localize pain. Imaging of high-risk areas, such as the abdomen, and areas of bruising or swelling may be required to exclude occult injuries. |
Table 75.3 Graded Assessment of Motor Function
| GRADE | ASSESSMENT ON PHYSICAL EXAMINATION |
|---|---|
| 0 | No active contraction |
| 1 | Trace visible or palpable contraction |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity |
| 4 | Movement against gravity and resistance |
| 5 | Normal power |
Table 75.4 Graded Assessment of Deep Tendon Reflexes
| GRADE | ASSESSMENT ON PHYSICAL EXAMINATION |
|---|---|
| 0 | Reflexes absent |
| 1 | Reflexes diminished but present |
| 2 | Normal reflexes |
| 3 | Reflexes increased |
| 4 | Clonus present |
Differential Diagnosis and Medical Decision Making
Indications for Cervical Spine Imaging
In the year 2000, in the hope of reducing the number of low-risk patients undergoing cervical spine plain film radiography, a multicenter study by the National Emergency X-radiography Utilization Study (NEXUS) group validated a set of five low-risk criteria for determining which patients do not require radiographic imaging if all the criteria are met (Box 75.1). This clinical decision tool demonstrated a sensitivity of 99.6% and a specificity of 12.9% for detecting clinically significant cervical spine fractures. It was thus extrapolated that 4309 (12.6%) of the 34,069 patients enrolled could have avoided plain film radiography.9
Box 75.1
NEXUS Low-Risk Criteria for a Cervical Spine Injury
1. No posterior midline neck pain or tenderness
2. No focal neurologic deficit
4. No evidence of intoxication
NEXUS, National Emergency X-radiography Utilization Study.
From Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med 2000;343:94-9.
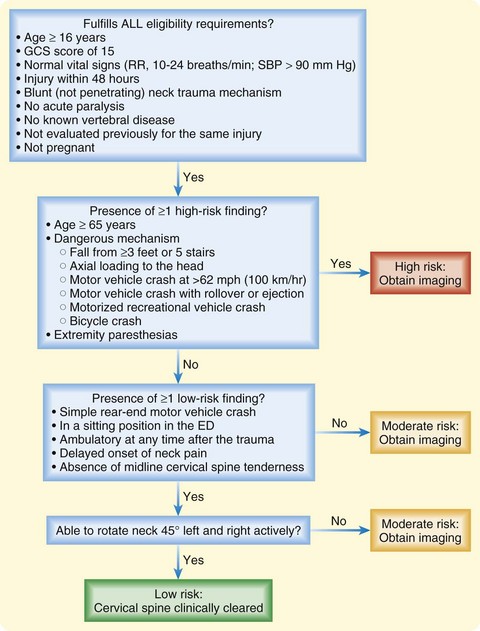
Following development of the NEXUS criteria, the Canadian Cervical-Spine Rule (CCR) was developed (Fig. 75.5). The validated sensitivity and specificity for this decision rule were 99.4% and 45.1%, respectively.10



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


