11 Spinal Cord Injuries in the Athlete Brian Kwon, David H. Kim, and Alexander R. Vaccaro Spinal cord injuries (SCIs) in athletes are uncommon and occur at an annual rate of 40 injuries per 1 million. These injuries are potentially devastating and particularly tragic when they occur in the setting of recreational or organized sports participation. SCIs occurring in sports typically involve the cervical spine during so-called collision sports, such as football and hockey (Table 11.1). The victims are characteristically young and healthy, and the injuries often result in permanent and significant disability or even death.1 The high-profile nature of organized sports in the United States has enhanced awareness of the potential for SCI, and many measures have been taken to reduce the risks of sustaining these injuries. Proper training and supervision of the athletes participating in high-risk sports have been shown to minimize the occurrence of injury to the head and neck during sports-related collisions. Due to such interventions and significant rule changes, the overall incidence of cervical SCI in both American football and North American hockey has significantly decreased over the past 30 years.2–4 Early injury recognition, appropriate stabilization of the injured athlete, and prompt treatment may improve the ultimate outcome following these injuries. SCIs that occur during sporting events are managed the same way as other traumatic cervical cord injuries. An organized system that includes personnel knowledgeable with the special requirements of protecting and mobilizing an athlete with potential SCI is essential. Over the past 30 years, sports participation has represented the fourth most common etiology of SCI and comprises between 10 and 15% of total SCIs. In the under-15-year age group, sports are the second most common etiology of SCIs. Males outnumber females 4:1, although this figure likely reflects the ratio of males to females involved in high-risk sports. For sports-related SCIs, the mean age at the time of injury is 24,5 significantly younger than the average age of 33 years for SCIs in general.1 Broken down by individual sporting events, diving accounts for the majority of SCIs, almost two thirds of the total sports-related injuries, followed by American football (Table 11.3). Figure 11.1 shows the overall distribution of SCIs. Figure 11.2 shows the distribution of SCIs by etiology in the under-15-year age group. Table 11.1 Spinal Cord Injuries in Sports
 Epidemiology (Table 11.2)
Epidemiology (Table 11.2)
Football (Table 11.4)
| Etiology | • Typically involve the cervical spine in collision sports |
| • Victims are often young and healthy | |
| • Injuries result in severe disability and even death | |
| Preventative measures | • Proper training |
| • Increased supervision | |
| • Rule changes | |
| Improving outcomes | • Early recognition of injury |
| • Appropriate stabilization | |
| • Prompt treatment | |
| • Organized system with knowledgeable personnel |
Historically, American football has been associated with a significant number of injuries in general and a relatively larger number of SCIs. However, there has been a dramatic decrease in the incidence of football-related SCIs in the past 30 years. The risk of neck injuries was noted during the initial organization of the sport. A further increase in the rate of injury was observed with the advent of the football helmet. First worn during the traditional Army-Navy game in 1893, the helmet was designed and implemented to protect players from head injuries. By 1940 both the National Collegiate Athletic Association (NCAA) and the National Football League (NFL) made its use mandatory. Despite this rule, serious head and neck injuries continued to plague the sport at all levels of play. In the 1950s, face masks were added to the helmet. Interestingly, the rate of head and neck injuries increased,6 as players may have felt more protected by face masks and became more apt to use their helmets and heads during high-risk blocking and tackling.
Table 11.2 Epidemiology of Spinal Cord Injuries in Sports
| Incidence rates | • Fourth most common etiology of SCIs |
| • Second most common etiology of SCIs in age group under 15 | |
| • 10 to 15% of total SCIs | |
| Gender differences | Male to female ratio 4:1 |
| Age | Mean age at time of injury = 24 |
| Sports | • Diving accounts for approximately two thirds of SCIs |
| • Football has next highest incidence |
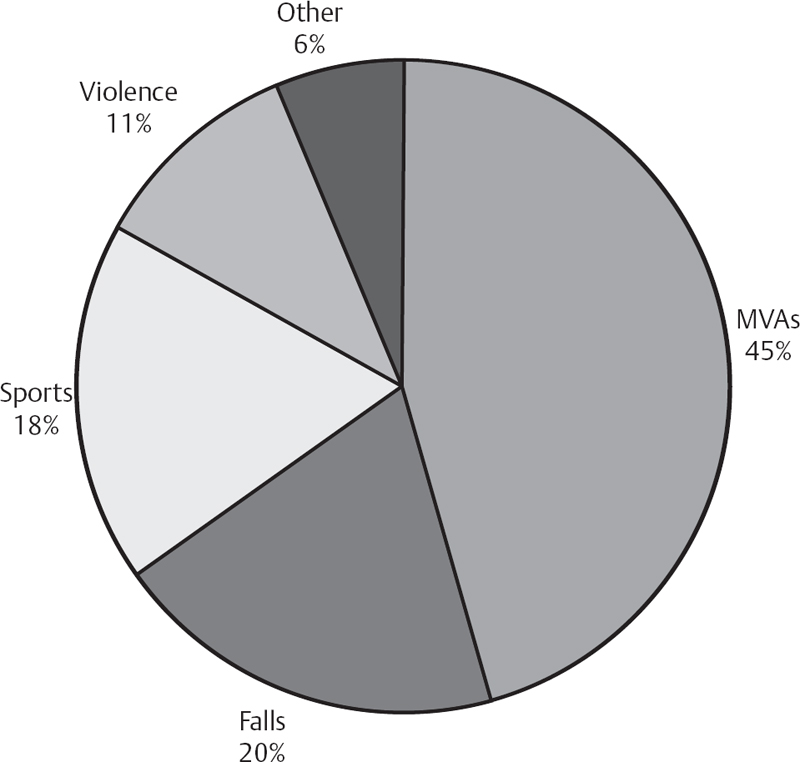
Fig. 11.1 Overall distribution of spinal cord injuries over a 30-year study period. MVAs, motor vehicle accidents.
| Etiology | Number | Percentage |
|---|---|---|
| Diving | 1601 | 65.4 |
| Football | 124 | 5.1 |
| Snow skiing | 118 | 4.8 |
| Horseback riding | 106 | 4.3 |
| Winter sports | 95 | 3.9 |
| Other sports | 80 | 3.3 |
| Surfing | 80 | 3.3 |
| Wrestling | 76 | 3.1 |
| Gymnastics | 47 | 1.9 |
| Field sports | 37 | 1.5 |
| Water skiing | 28 | 1.1 |
| Baseball | 19 | 0.8 |
| Rodeo | 18 | 0.7 |
| Basketball | 10 | 0.4 |
| Track and field | 5 | 0.2 |
| Skateboard | 4 | 0.2 |
| Total | 2448 |
Source: From the National Spinal Cord Injury Statistical Center, University of Alabama at Birmingham, Annual Statistical Report, July 2005.
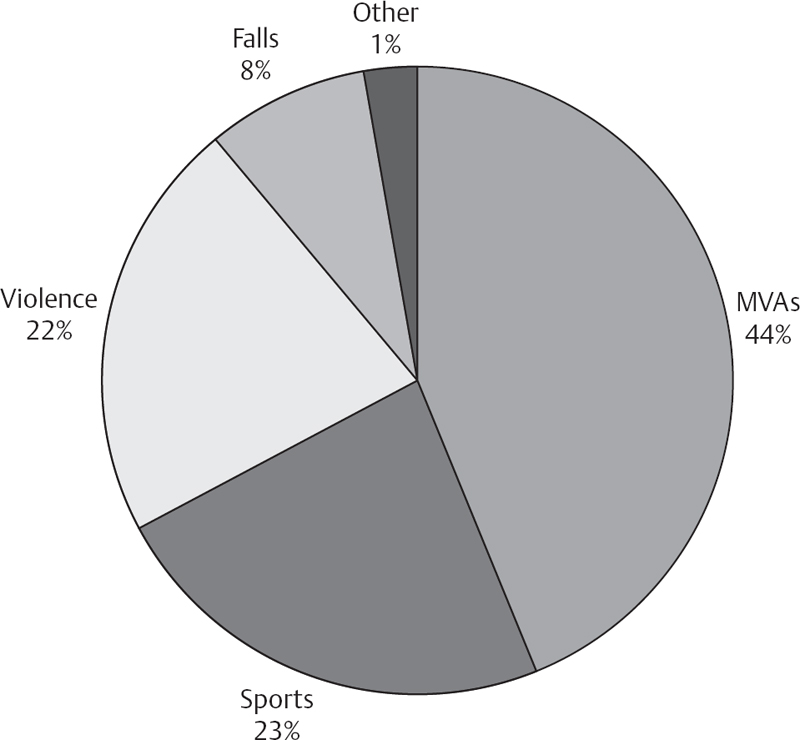
Fig. 11.2 In the under-15-year age group, sports injuries are the second most common etiology of spinal cord injuries.
Dr. Joseph Torg et al7 developed a registry to record and monitor serious cervical spine injuries occurring during football games. The ensuing observations and reports led to significant rule changes that prohibited players from using their helmets as blocking and tackling mechanisms or as projectiles. The NCAA and the National Federation of State High School Associations disallowed so-called spearing maneuvers in which the crown of the head is used during blocking and tackling.8
Table 11.4 Football-Related Spinal Cord Injuries
| Evolution | • Neck injuries noted during initial organization of the sport |
| • Introduction of helmet wear led to an increase in rate of injury | |
| • Many feel these increases are a result of players feeling more protected, so are more apt to use helmets during blocking and tackling | |
| Torg et al7 | • Developed sports registry to record cervical spine injuries |
| • National Center for Catastrophic Sports Injury Research | |
| • “Spearing” (tackling by leading with one’s head) made illegal by NCAA and high school sports associations | |
| Cantu and Mueller3 | • Observations from 1977 to 2001 |
| • Total 223 SCIs | |
| • Incidence of SCIs increased with increased speed, forces, and level of play | |
| • SCIs observed (per 100,000): | |
| • 0.52 = high school | |
| • 1.55 = college | |
| • 14.0 = professional | |
| Boden et al9 | • Observations from 1989 to 2002 |
| • Showed significant increase in football-associated SCIs | |
| • Overall incidence spine injuries (per 100,000): | |
| • 1.10 = high school | |
| • 4.72 = college | |
| • Incidence of quadriplegia (per 100,000): | |
| • 0.50 = high school | |
| • 0.82 = college | |
| • Approximately six quadriplegic injuries per year | |
| • Most injuries occur while playing defense (57.5%) and making tackles (79.7%) | |
| • 43 cases of cervical cord neurapraxia (CCN) | |
| • None suffered SCI | |
| • Incidence of CCN (per 100,000): | |
| • 0.17 = high school | |
| • 2.05 = college | |
| Efforts to reduce incidence of SCI | • Coaches urged to enforce illegal nature and danger of spearing |
| • Concentrate on teaching proper tackling technique | |
| • Physical conditioning (pericervical musculature) |
Cantu and Mueller3 reported on catastrophic cervical spine injuries from 1977 to 2001, the 25 years following implementation of the aforementioned rule changes. They studied data from the National Center for Catastrophic Sports Injury Research at the University of North Carolina at Chapel Hill, which collects reports from physicians treating injured athletes on the high school, collegiate, and professional levels. The study reported a total of 223 cervical spine injuries in which no or incomplete neurologic recovery was documented. There were 183 injuries in high school players, 29 in college athletes, and 7 in professional athletes. When factoring in the number of participants at risk, the incidence of catastrophic SCIs appeared to increase in direct association with the increased speed, forces, and level of play. SCIs observed, per 100,000 participants, were 0.52 at the high school level, 1.55 in college athletes, and 14.0 at the professional level.
Subsequently, Boden et al9 published an updated report from the National Center for Catastrophic Sports Injury Research on data collected between 1989 and 2002. These figures suggest that there has again been a significant increase in the rate of football-associated SCIs. During the time period of the study, the overall incidence of cervical spine injuries was 1.10 per 100,000 high school athletes and 4.72 injuries per 100,000 college participants. The incidence of quadriplegia in high school and college was 0.50 and 0.82 injuries per 100,000 athletes, respectively. There were 76 quadriplegic injuries sustained, leading to an overall incidence of approximately 6 per year in scholastic football. The mean age of the players at the time of injury was 17 years. Most injuries occurred while playing on defense (57.5%) and making a tackle (79.7%). The expert opinion in most cases, including four cases documented on videotape, was that the mechanism of injury involved spear tackling.
In the same study,9 there were also 43 reported episodes of cervical cord neurapraxia (CCN). The calculated mean incidence of CCN in college players was 2.05 per 100,000 participants and 0.17 per 100,000 high school participants. Two players reported a previous episode of CCN, and none of the 43 players suffered permanent quadriplegia during the study period. It is likely that these figures represent an underestimate of the true incidence of CCN in organized football and that cases are not reported at the same rate as more significant SCIs.
Despite widespread belief that the number of SCIs has decreased over time, as seen by most recent data, there has been an apparent increase in the rate of these injuries. Coaches have been urged to enforce the illegal nature of and dangers involved in spear tackling. Proper tackling technique and physical conditioning, particularly of the pericervical musculature, have been strongly encouraged. The NCAA, effective for the 2005–2006 academic year, removed the term intentional from the spearing rule in efforts to strengthen the wording. This may give referees freedom to call the penalty more often as they would not have to judge intent.3,9,10 Of note, there were 18 lawsuits or insurance settlements associated with the injuries included in the most recent study by Boden et al.9
Ice Hockey (Table 11.5)
Ice hockey in North America has undergone increased scrutiny because of the regular occurrence of high-profile cases of quadriplegia. In 1981 a registry to document and track SCIs due to ice hockey was created. Following the creation of the Committee on Prevention of Spinal Cord Injuries Due to Hockey, an abrupt increase in SCIs was noted in the late 1980s. It was not known at the time whether this was due to better reporting and awareness or to a true increase in the rate of SCIs. A report following evaluation of the initial data did not provide much in the way of conclusions other than the suggestion that SCIs occurring during ice hockey were multifactorial and worthy of study.11,12
Table 11.5 Ice Hockey-Related Spinal Cord Injuries
| Committee on Prevention of SCIs Due to Hockey | • Created in 1981 |
| • Abrupt increase in SCIs seen in the late 1980s; could be from better reporting and awareness or actual increase | |
| Tator et al4 | • 271 reported SCIs between 1943 and 1999 in Canada |
| • 49% between ages 16 and 20 years | |
| • Mean age at time of injury = 20.6 years | |
| • Injury mechanisms: | |
| • Striking boards with head = 67% | |
| • Checked from behind = 37% | |
| • Checked (not from behind) = 24% | |
| • 83.0% involved cervical spine, 47.3% sustained permanent neurologic loss | |
| Increased incidence | • Increased speed and size of players |
| • More aggressive risk-taking behavior (based on psychosocial profile) | |
| • False sense of security with helmet wear |
Tator et al4 reviewed reports of 271 SCIs documented between 1943 and 1999 in Canada. The 16- to 20-year-old age group was most frequently affected and comprised 49% of the total. The overall mean age at the time of injury was 20.6 years. The injury mechanism in the majority of cases involved a player striking the boards with his head (67%), and the most frequent cause was being pushed or checked from behind by another player (37%) and being checked but not from behind (24%). The cervical spine was involved in 83.0% of injuries, and 47.3% of players sustained permanent neurologic losses. The overwhelming majority of injuries (91%) occurred during supervised games.
An increase in the speed and physical size of players may account to some degree for observed increases in the rate of spinal injuries. Recommendations have been made to change the rules and enforce penalties for illegal techniques, such as checking a player from behind. Possible changes in equipment have been proposed, such as rounding the helmet tops. More importantly, changing attitudes about smart play have begun. As previously suggested, the use of helmets has lowered rates of head injury but may also give athletes a false sense of security and lead to more aggressive, less protected behavior.4,11 A study of the psychosocial profiles of hockey players has also suggested that aggressive, risk-taking behaviors contribute directly to a higher incidence of spinal injury.12
Rugby (Table 11.6)
Another popular sport with relatively high rates of SCI is rugby. Although there are several rule variations, all versions of the sport involve high-velocity collisions between players who wear relatively little or no protective gear. Several authors have studied SCIs that occur in the Rugby Union and Rugby League in Australia, New Zealand, and Ireland.8,13–15 In each study, a relatively constant high rate of SCI was identified spanning several years.
Overall, the Rugby Union had the highest incidence of SCIs. Between 1986 and 1991 there were 9.2 reported cases of SCI per 100,000 players. Between 1995 and 2003 the rate decreased somewhat to 6.8 injuries per 100,000. This decrease, however, was not significant. During the same time periods the rate of SCI per 100,000 players in the Rugby League, which has several rule differences with the Rugby Union, were 2.3 and 1.7, respectively. The difference was significant. The majority of injuries in union players occurred during the scrum, whereas in league players they tended to occur during tackling. This difference is felt to be due to major rule differences governing the scrum between union play and league play. Among 31 injuries in the Rugby Union reported by Berry et al,14 11 were caused by scrums, and 9 were caused by tackling, with both representing 64% of the total injuries observed. In the Rugby League, Berry et al reported 1 SCI during the scrum and 18 during tackling, with both mechanisms making up 82% of the injuries in league play.
In the Rugby Union a scrum involves eight players lined up in a 3-4-1 formation. The scrum occurs after specific events, such as accidental offsides, rucks (group tackles), and mauls (group tackles where the player stays standing and the referee whistles the ball dead). In the Rugby League the scrum is reduced in power by involving fewer players (six in a 3-2-1 pattern) and does not allow for any pushing or contesting. Although likely reducing the risk of injury during the scrum, this form of scrummage has been criticized as not embodying the true nature of the scrum. Efforts to enforce stricter scrummage regulations have been resisted, as teams continue to attempt to gain tactical advantage in recovering the ball during this phase of the game by thrusting and engaging opponents as forcefully as possible. One of the goals of the scrum quoted on a Web site was explicitly stated as follows: “to push the other side off the ball or at least break the opposing hooker/prop’s neck/spine.”
Table 11.6 Rugby-Related Spinal Cord Injuries
| Incidence rates | • Highest rates of SCI were seen in Rugby Union (as opposed to Rugby League) |
| Rugby Union (per 100,000): | |
| • 1986–1991 = 9.2 cases | |
| • 1995–2003 = 6.8 cases | |
| Rugby League (per 100,000): | |
| • 1986–1991 = 2.3 cases | |
| • 1995–2003 = 1.7 cases | |
| Rugby League vs Rugby Union | • Rule differences between the two specifically regarding the scrum |
| • Scrummage injuries: | |
| • Rugby Union = 11/31 cases | |
| • Rugby League = 1/19 cases (18/19 during tackling) | |
| • Efforts to enforce stricter regulations have been resisted |
In a cadaver study modeling scrums, the horizontal force during initial contact was measured at 4.4 kilonewton (kN) to 8 kN,16 which exceeds the upper limit of the axial load required to cause compression failure of the cervical spine.11 Not surprisingly, several health care officials have called for governmental-level changes in the rules of rugby, stating that to allow players, particularly schoolboys, to continue with the current rules “constitutes culpable negligence.”15
Table 11.7 Water Sports-Related Spinal Cord Injuries
| Incidence and causes | Diving is leading cause of SCIs; represents two thirds of all such injuries |
| Demographic and temporal pattern17 | • Average age of 23 |
| • Occurred between May and September | |
| • Reckless behavior, ignorance, and alcohol were all factors |
Water Sports (Table 11.7)
Diving is the leading cause of SCIs related to sports and leisure activities and represents the cause of nearly two thirds of all such injuries.1,17 SCIs from diving accidents occur to a distinct demographic and in a specific temporal pattern. A recent review by Korres and colleagues17 retrospectively reviewed SCIs due to diving accidents. They found 20 patients (19 males and 1 female) whose average age was 23 years at the time of injury. All injuries occurred between May and September. They found reckless behavior, ignorance, and alcohol use in young males to be the typical factors in those injured. Poor judgment and diving head first into shallow pools were the most frequently reported injury mechanisms.
Tumbling Sports (Table 11.8)
Cheerleading has developed into a competitive sport and as such has experienced progressive increase in the apparent rate of injuries resulting from more acrobatic high-energy maneuvers. Over a 17-year period from 1983 to 2000, cheerleading accounted for almost half of the serious cervical spine injuries in women. The rate of these injuries over that time period was 1.03 per 100,000 participants. New rules have changed the methods and height at which the cheerleaders can be catapulted into the air, and it is hoped these rules will lead to fewer catastrophic injuries.18
Skiing/Snowboarding (Table 11.8)
Skiing and snowboarding accidents are a major concern due to the very high volume of participants, estimated at 14 million in the United States and over 200 million worldwide.18 Although most serious injuries are head injuries, spine injuries also occur at a reported incidence of 1 per 100,000 skier days and 4 per 100,000 snowboarder days. In contrast to other sports activities, most spine injuries occurring in association with skiing and snowboarding are thoracolumbar injuries.18 Specific data regarding the rates of cervical spine and SCI are unavailable.
 Injury Syndromes (Table 11.9)
Injury Syndromes (Table 11.9)
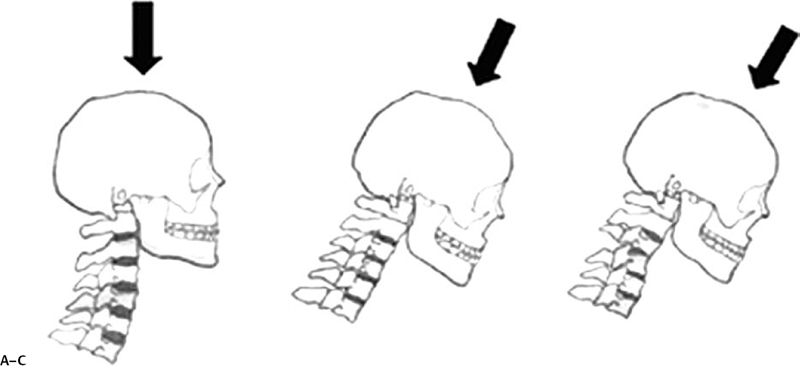
Cervical SCIs occur when the athlete’s head is rapidly decelerated against an immobile object. The head is fixed in position, and the cervical spine becomes an intervening mobile segment between the head and the body. The momentum of the body contributes a significant axial load during its deceleration. The resulting injury pattern depends in part on the position of the neck at the time the axial load is applied. When the neck is in a neutral or lordotic position, axial loads can be dissipated by paraspinal musculature and ligamentous structures. However, when the neck is flexed, lordosis is eliminated, and the cervical spine then behaves biomechanically like a rigid column (Fig. 11.3). Axial loads are dissipated through the bony structures, resulting in significant force transfer.2
Table 11.8 Tumbling Sports- and Skiing/Snowboarding-Related Spinal Cord Injuries
| Tumbling sports | • 1983–2000: cheerleading was almost one half of cervical spine injuries in women |
| • Rule changes, including height at which cheerleaders can be catapulted, may reduce incidence | |
| Skiing/snowboarding | • Major concern due to high volume of participants |
| • 14 million in United States, > 200 million worldwide | |
| • Spine injury incidence (per 100,000 skier days): | |
| • Skiers = 1 | |
| • Snowboarders = 4 | |
| • Most injuries are thoracolumbar injuries |
Torg et al19 have also examined the mechanism by which football players suffer cervical SCIs. As previously noted, a majority of such injuries occur during tackling, particularly with the head in the down position. This observation gave rise to the “nose-to-the-numbers” technique of tackling that is currently being taught. Many authors have urged coaches and trainers to emphasize the importance of these principles during play.3,9
| Cervical SCI mechanisms | • Occur when head is rapidly decelerated against immobile object |
| • Cervical spine becomes intervening mobile segment between head and body | |
| • Injury pattern depends on neck position at time axial load is applied | |
| • Neutral, lordotic position: axial loads dissipated by paraspinal musculature and ligaments | |
| • Flexed position: cervical spine becomes rigid column, with axial loads dissipated through bony structures | |
| Transient neurapraxia | • “Burners” (stingers): benign events from stretch injury to upper roots and trunks of brachial plexus or foraminal compression of nerve roots |
| • Radiating pain down one extremity (if bilateral, could be more serious) | |
| • Return to play if symptoms quickly resolve with no strength deficits or limitations in range of motion | |
| • MRI or EMG if symptoms persist after 2 to 4 weeks | |
| • “Burning hands syndrome”: variant of central cord syndrome and implies actual SCI | |
| Cervical cord neurapraxia (CCN) | • Definition: temporary paralysis lasting for 15 minutes and up to 48 hours, followed by full recovery |
| • Torg ratio: sagittal diameter of spinal canal/sagittal diameter of vertebral body | |
| • Smaller Torg ratio (< 0.8, normal = 1.0) does not predict catastrophic SCI and should not prevent a player from participating | |
| Spear-tackler’s spine | • Constellation of radiographic findings: |
| • Developmental cervical stenosis | |
| • Persistent straightening or loss of normal cervical lordosis | |
| • Persistent radiographic evidence of previous injury | |
| • Clinical history of previous use of spear tackling | |
| • Absolute contraindication to participation in collision sports |
Transient Neurapraxias
“Burners” (also known as “stingers”) are relatively benign events that are thought to arise from a stretch injury to the upper roots and trunks of the brachial plexus or foraminal compression of the existing nerve roots. Players often experience radiating pain down one extremity. Bilateral stingers are less benign and may represent a potentially more significant injury involving the cervical spinal cord. Associated weakness, especially of the deltoid, biceps, and spinatus muscles, can occur and should be specifically tested for on the sidelines. Athletes can return to play if symptoms quickly resolve and there are no strength deficits and sensory changes and no limitation to neck range of motion.
Persistent symptoms from a stinger should warrant advanced imaging with magnetic resonance imaging (MRI) to look for possible cervical disk herniation, cervical stenosis, cord compression, or signs of actual cord injury. Electromyography (EMG) performed 2 to 4 weeks after injury can be helpful. Typical findings include a mild conduction block, but sharp waves and fibrillation potentials can also be seen. Even with abnormal EMG findings, athletes can return to play if symptoms resolve. However, persistent sensory symptoms or muscle-specific weakness with concordant EMG changes should preclude a player from returning to play in contact sports.11,20
“Burning hands” syndrome is an entirely different diagnosis. It is considered a variant of central cord syndrome and implies actual SCI. Radiographic evidence of cervical spine injury can be seen in up to 50% of cases.