CHAPTER 18
Sphenopalatine Ganglion Block
INDICATIONS
The sphenopalatine ganglion (SPG) is a large extracranial structure that has rich sympathetic and parasympathetic autonomic innervations, which explains the autonomic features associated with cluster headache. Cluster headache involves activation of the parasympathetic outflow from the superior salivary nucleus of the facial nerve, predominantly through the SPG.1
• SPG block and radiofrequency ablation (RFA) are indicated in the management of intractable medically resistant cluster headaches, migraine, and other trigeminal autonomic cephalalgias.
• Intractable orofacial pain syndromes (eg, persistent idiopathic facial pain, “atypical facial pain”).
SPHENOPALATINE GANGLION NEUROANATOMY
The SPG has rich parasympathetic (preganglionic axons and postganglionic cell bodies and axons) and sympathetic (postganglionic axons) components. The parasympathetic preganglionic cell bodies projecting to the SPG originate in the superior salivatory nucleus (SSN) of the facial nerve in the pons.
The efferent fibers of the SSN travel in the nervus intermedius and divide at the geniculate ganglion to become the greater petrosal nerve and chorda tympani nerve. The first-order parasympathetic neurons in the greater petrosal nerve are joined by the postganglionic sympathetic fibers from the deep petrosal nerve, forming the nerve to the pterygoid canal (vidian nerve). The preganglionic parasympathetic neurons then synapse with the second-order parasympathetic neuronal cell bodies located in the SPG.
The postganglionic parasympathetic fibers then run with branches of the maxillary nerve (V2) to reach their targets. Therefore, the only cell bodies located within the SPG are those of the second-order postganglionic parasympathetic neurons, which may explain the clinical observation that patients after radiofrequency ablation (RFA) of the SPG usually notice improvement of the autonomic parasympathetic symptoms either earlier or even without improvement of the headache pain.
The sympathetic cell bodies projecting to the SPG originate in the upper thoracic spinal cord (T1-T2). The preganglionic sympathetic neurons then synapse in the cervical sympathetic ganglia, mainly the superior cervical ganglion. The postganglionic second-order sympathetic neurons form the carotid sympathetic plexus and reach the pterygoid canal through the deep petrosal nerve where it joins the first-order parasympathetic neurons in the greater petrosal nerve, forming the nerve to the pterygoid canal (vidian nerve). Postganglionic sympathetic fibers pass through the SPG without synapsing and innervate mainly the blood vessels.
SPHENOPALATINE GANGLION ANATOMY
The SPG is located in the pterygopalatine fossa (PPF), which is a small, upside-down pyramidal space 2 cm high and 1 cm wide.
• The pterygopalatine fossa is located behind the posterior wall of the maxillary sinus and is bordered posteriorly by the medial plate of the pterygoid process, superiorly by the sphenoid sinus, medially by the perpendicular plate of the palatine bone, and laterally it communicates with the infratemporal fossa.
• Superolaterally lies the foramen rotundum with the exiting maxillary nerve, and inferomedially there is the vidian nerve (greater petrosal and deep petrosal nerves) within the pterygoid canal (Table 18-1).
• The pterygopalatine fossa contains the internal maxillary artery and its branches, the maxillary nerve, and the SPG and its afferent and efferent branches.
• The SPG is located posterior to the middle turbinate and is few millimeters deep to the lateral nasal mucosa.
• It is suspended from the maxillary nerve by the pterygopalatine nerves, inferiorly it is connected to the greater and lesser palatine nerves, and posteriorly it is connected to the vidian nerve.
• Efferent branches of the SPG form the posterior lateral nasal and pharyngeal nerves.2,3
TABLE 18-1. The Pterygopalatine Fossa Foramina and Connections
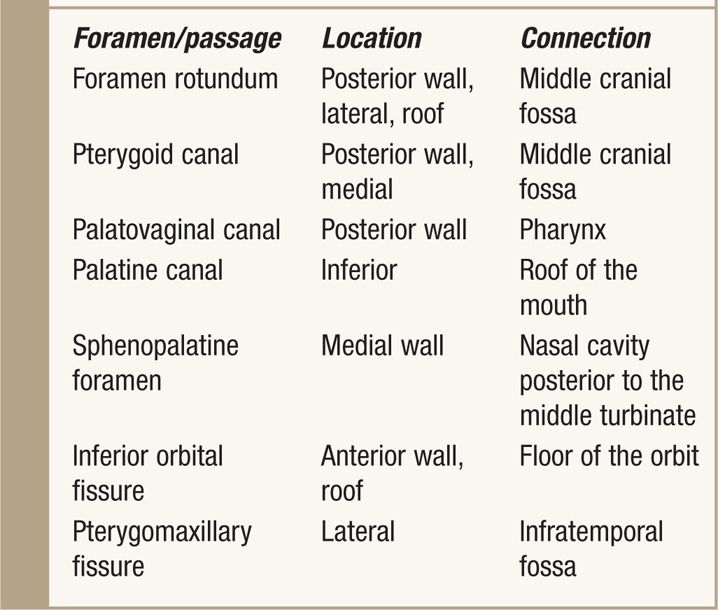
The key to successfully locating the pterygopalatine fossa lies in identifying its boundaries:
• Anterior. Superomedial part of the infratemporal surface of maxilla.
• Posterior. Root of the pterygoid process and adjoining anterior surface of the greater wing of sphenoid bone.
• Medial. Perpendicular plate of the palatine bone and its orbital sphenoidal processes.
• Lateral. Pterygomaxillary fissure.
• Superior. Sphenoid sinus.
• Inferior. Part of the floor is formed by the pyramidal process of the palatine bone.
The key to successfully locating the pterygopalatine fossa by lateral x-ray view lies in identifying the following structures:
• Maxilla anteriorly
• Lateral pterygoid plate posteriorly
• Coronoid notch of the mandible (for the transcoronoid needle approach)
BASIC CONCERNS AND CONTRAINDICATIONS
As with any intervention, one must weigh the potential benefits to the potential risks. Given the relatively invasive nature of the procedure, sphenopalatine ganglion blockade/neurolysis should be considered only in intractable, medically resistant cluster/migraine headache and neuropathic face pain disorders.
• Immunocompromised patients are potentially at high risk for infection; this is of particular relevance in patient with facial malignancy.
• Infection, systemic or localized.
• Coagulopathy and thrombocytopenia.
• Distorted or complicated anatomy.
• Patient refusal.
PREOPERATIVE CONSIDERATIONS
• Informed consent and proper explanation of all potential complications.
• Anticoagulation. It is essential to review the patient’s medications and obtain international normalized ratio/prothrombin time and platelet counts when appropriate as there is a possibility of injury to the maxillary artery or branches.
• Physical examination of the area for infection.
• Intravenous access for IV fluid and medications for sedation or to manage complications should any arise.
• Evaluation for contrast allergy. This is important as the utilization of contrast will allow for precise needle placement in the PPF and to role out intravascular injections.
Fluoroscopic Views
• Lateral view. This is most important view in identifying the PPF. This view should be the starting view to identify the maxilla, lateral pterygoid plate and the coronoid notch. A slight tilt will allow for proper overlapping of the pterygoid plates for proper visualization of the fossa (Figures 18-1 and 18-2).
• Anterior-posterior (AP) view. Once the needle is placed in the proper direction with the lateral fluoroscopy, the physician should immediately shift to the AP view as it allows to control the depth of the needle tip as it advances toward the lateral nasal wall (Figure 18-3).

Figure 18-1. Lateral x-ray showing SPG block with the anterior approach. Please note that the x-ray cursor is overlying the coronoid notch. (Reproduced with permission from Ohio Pain and Headache Institute.)
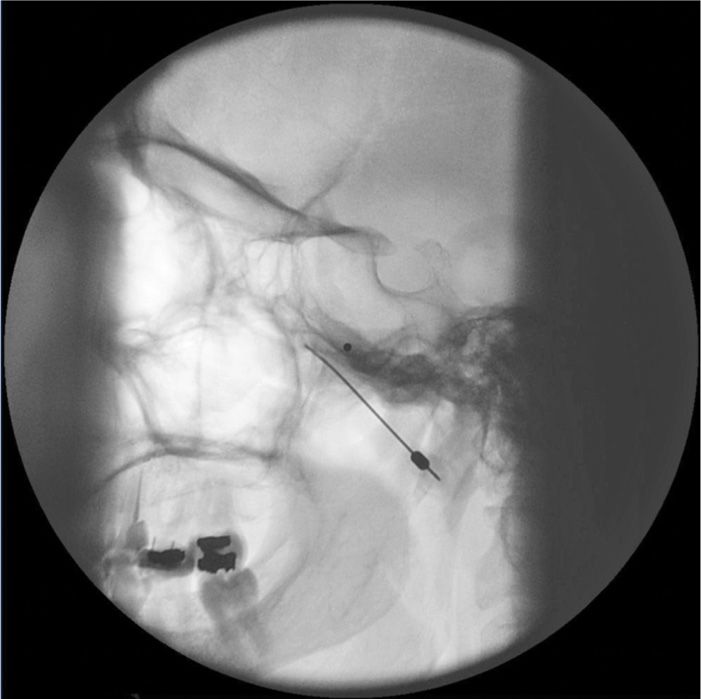
Figure 18-2. Lateral x-ray showing SPG block with the coronoid approach. (Reproduced with permission from Ohio Pain and Headache Institute.)

Figure 18-3. AP x-ray view showing the needle tip just lateral to the nasal wall. The contrast agent is delineating the PPF. (Reproduced with permission from Ohio Pain and Headache Institute.)
Equipment
• Pointer and skin marker
• 25-gauge 1.5-in needle (local needle)
• 22-gauge 3.5-in blunt Tuohy needle (block needle)
• 3- or 5-cc syringe for local anaesthetic
• 1- or 3-cc syringe for contrast
• 3- or 5-cc syringe for medications
• Exrension tubing
Medications
• 5-mL 1% lidocaine
• 3-mL 0.25% or 0.5% bupivacaine
• 1-mL Iohexol 180 (nonionic water-soluble contrast)
• Triamcinolone (preferred as it is nonparticulate) or methylprednisolone
APPROACHES TO THE SPHENOPALATINE GANGLION
Transnasal Approach
As the SPG is located couple of millimeters deep to the lateral nasal mucosa, topical application of local anesthetic solution to the posterior wall of the nasopharynx in the region of the middle turbinate can diffuse across the nasal mucosa to block the SPG.
Transnasal blockade of the SPG was first reported using topical cocaine4; currently lidocaine 4% is usually used.
• The patient is placed in the supine position with the neck extended into a sniffing position.
• 10-cm cotton tipped applicator soaked with 4% lidocaine is slowly advanced along the superior border of the middle turbinate until it reaches the posterior wall of the nasopharynx.
• The applicator is usually left in place for approximately 20 to 30 minutes to allow the local anesthetic to diffuse across the mucosa and reach the SPG.
Transnasal Endoscopic Approach
This endoscopic technique for transnasal injection and blockade of the SPG was first described by Prasanna in 1993.5 This technique allows a needle to be inserted transnasally under vision through the sphenopalatine foramen into the PPF.
Transoral Approach
The pteygopalatine fossa can also be accessed transorally by placing a 27-gauge needle inside the greater palatine foramen. This approach is usually utilized by dentists to block the palatine nerves.6
Infrazygomatic Approach
Neuroablation techniques are only feasible with this infrazygomatic approach. Needle placement is usually guided by fluoroscopy; however, CT guidance is reported as well.7
The infrazygomatic approach could be either anterior to the mandible or through the coronoid notch of the mandible.
Anterior approach. The needle entry is inferior to the zygomatic arch, just anterior to the mandible, between the mandibular ramus and the posterior border of the zygomatic bone. We prefer this approach as the needle can be advanced in a target view toward the PPF without the need to walk the needle off the lateral pteygoid plate (which is usually very painful) (Figure 18-1). Also it is much easier to steer the needle (cephalad-caudad or anterior-posterior) within the fossa to selectively target different structures within the fossa. However, this approach is not feasible in all patients as there might not be enough room between the mandible and the zygoma to insert the needle.8
Coronoid approach. The needle entry is through the coronoid notch of the mandible. The needle is usually advanced to target the lateral pterygoid plate first and then walked off the bone interiorly to enter the PPF. By that time, the needle usually acquired certain direction and it is hard to manipulate the needle once it is inside the fossa (Figure 18-2).
Technique of SPG Block (Infrazygomatic Approach)
• With the patient in the supine position and the head inside the C-arm, a lateral view is obtained and either the C-arm or the head of the patient is rotated until both pterygoid plates are superimposed on each other to better visualize the pterygopalatine fossa.
• The skin entry site overlying the fossa is marked just inferior to the zygomatic arch either anterior to the mandible (anterior approach, my preferred approach) or through the coronoid notch (transcoronoid approach).
• A 22-gauge, 3.5-in blunt needle with a slight bend at the tip is used.
• The needle is first introduced in the lateral view and advanced medially and superiorly toward the pterygopalatine fossa using real-time fluoroscopy.
• Once in a proper direction, an anteroposterior view is obtained, and the tip of the needle is advanced to be just lateral to the nasal wall (Figure 18-3).
• If the lateral pterygoid plate is encountered, the needle should be walked off the bone anteriorly and cephalad to slip into the fossa (the curved tip will help to guide the needle).
• 0.1 to 0.2 mL of contrast agent is injected under real-time fluoroscopy to rule out intravascular spread as the PPF contains the maxillary artery and its branches (mainly the sphenopalatine artery).
• After negative aspiration of blood or air (the needle tip is too advanced into the nasal cavity or the maxillary sinus), 1 to 2 L of 0.5% bupivacaine with or without steroids is injected slowly.
POSTPROCEDURE FOLLOW-UPS
The patient should be monitored in the recovery room for 40 to 60 minutes for any signs of bleeding or unexpected neurologic symptoms/signs. Patient should be advised to call pain service for any procedure-related complications and/or any unexpected neurologic deficit. Patient should be monitored closely for the following:
• Bleeding, epistaxis
• Facial numbness or weakness
• Double vision
• Fever
• Exacerbation of symptoms
• Headache side shifts
Radiofrequency Ablation Technique
• With the patient in the supine position and the head inside the C-arm, a lateral view is obtained and either the C-arm or the head of the patient is rotated until both pterygoid plates are superimposed on each other to better visualize the pterygopalatine fossa.
• The skin entry site overlying the fossa is marked just inferior to the zygomatic arch either anterior to the mandible or through the coronoid notch.
• A 22-gauge, 10-cm, blunt RFA needle with a 2-mm or 5-mm active tip with a slight bend at the tip is used (Figure 18-4). The needle is first introduced in the lateral view and advanced medially and superiorly toward the pterygopalatine fossa using real-time fluoroscopy.
• Once in a proper direction, an anteroposterior view is obtained, and the tip of the needle is advanced to be just lateral to the nasal wall.
• If the lateral pterygoid plate is encountered, the needle should be walked off the bone anteriorly and cephalad to slip into the fossa (the curved tip will help to guide the needle).
• Sensory stimulation is obtained with 50 Hz to look for deep paresthesias behind the root of the nose at >0.5 V (Table 18-2).
• Once proper stimulation is achieved and prior to lesioning, 0.1 to 0.2 mL of contrast agent is injected under real-time fluoroscopy to rule out intravascular spread.
• Then, 0.5 mL of lidocaine 2% is injected and two radiofrequency lesions are carried out at 80°C for 60 seconds each.
• After lesioning, 0.5 mL of bupivacaine 0.5% and 5 mg of triamcinolone are injected with the aim to prevent postprocedure neuritis.9

Figure 18-4. Lateral x-ray view showing the RFA needle inside the PPF. Note that the tip is curved downward to avoid lesioning of the naxillary nerve which runs at the roof of the PPF. (Reproduced with permission from Ohio Pain and Headache Institute.)
Related posts:
 Corticosteroids: Inditoc-authortions, Pharmacology, and Risks in Interventional Pain Management
Corticosteroids: Inditoc-authortions, Pharmacology, and Risks in Interventional Pain Management
 Surgical Treatment of Trigeminal Neuralgia
Surgical Treatment of Trigeminal Neuralgia
 Sacroiliac Joint Injections
Sacroiliac Joint Injections
 Supraclavicular and Infraclavicular Nerve Blocks
Supraclavicular and Infraclavicular Nerve Blocks
 Commercially Available Reservoir Options for Intrathecal Drug Delivery
Commercially Available Reservoir Options for Intrathecal Drug Delivery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


