15 Socioeconomics of Spinal Injuries Rob D. Dickerman, Michael O’Malley, and Jack E. Zigler The annual incidence of spinal cord injuries (SCIs) in the United States is approximately 40 cases per 1 million population, resulting in 11,000 new cases per year.1 The costs to the patient, family, and society are staggering, with the lifetime costs for a tetraplegic patient injured at age 25 years closely approximating $3 million.2 According to the Centers for Disease Control and Prevention (CDC), SCIs cost the nation an estimated $9.7 billion each year. Pressure sores alone, a common secondary condition among people with SCI, cost an estimated $1.2 billion.3 As stated by Formal et al,4 economic costs of SCI are high, as seen in charges that can amount to approximately $350,000 for those with high tetraplegia in the first year alone. To break it down further, medical costs for the average SCI average $200,000 in the first year and $25,000 each year thereafter. Societal costs remain very high, as life expectancy rates increase, with direct costs amounting to $2.7 billion and indirect costs at $3.7 billion.5 Several studies were conducted in the 1990s on the direct and indirect costs of SCI to the patient and society, with varying results and estimations.6,7 The main source of spinal cord injury data in the United States is the National Spinal Cord Injury Statistical Center (NSCISC). Since 1989, NSPISC has collected data on SCI patients from the 18 regional Model Spinal Cord Injury Care Systems located throughout the United States the NSCISC collects on injury severity, hospitalization and inpatient rehabilitation period, postdischarge rehabilitation, and mortality. This chapter reviews the costs, to both the patient and society, of SCI in the United States and Canada. Both the acute and rehabilitation care stages for the SCI patient place a significant financial strain on society due to the “intensive resources” needed for patient management.8 In addition, life expectancy postinjury continues to increase, further increasing the financial burden that is associated with continued care of an SCI patient. To achieve some perspective of this cost of care, insight on the care and rehabilitation programs set in place at the time of, and following, patient assessment is necessary.9 Rehabilitation consists of certain objectives, including but not limited to maximizing patient medical and functional outcomes, as well as educating both patient and family on the current situation and what is required of them during the long road ahead. This can only be accomplished via initial and continuing patient assessment by a team of physicians, therapists, psychologists, social workers, and case managers. Realistic functional outcomes must also be predicted and discussed. Only then can the patient, family, and rehabilitation team begin to work on attaining these functional goals. With regard to the education and information needs of SCI patients and their families, Burkell et al10 state that self-directed care is an integral aspect of health for those living with a chronic illness or disability. Not only is it important to realize that one’s health care needs change over time, but studies have shown that the need for information regarding prevention, identification, and treatment of SCI actually increases with time. Thus, the comprehensive education that patients and families receive during initial contact with the health care team must be carried over, and must evolve with the patients’ course of care. The timely and precise nature of information delivery remains a significant challenge. Internet use is becoming more common, but the most used information source remains periodicals (journals, newsletters, etc.). Advances in information accessibility could significantly decrease SCI costs, as many of the common complications, such as pressure sores and urinary tract infections, can be avoided given appropriate self-care measures.10 The severity of spinal cord injuries varies, as does the cost of care for each patient. Complete SCI refers to those injuries resulting in complete loss of motor and sensory function below the site of injury. Patients with incomplete SCI retain some function below the level of injury, whether it is sensory, motor, or both.3 Those with more severe injuries generally require more health and rehabilitation services.10 Table 15.1 lists the levels of functional dependence on others, as well as the need for assistive devices, wheelchairs, and specialized cars, all of which add to the burden of cost for these patients. Technologic advancements have enhanced the functional capabilities of patients, but not without a cost. Assistive devices, orthotics, surgical reconstruction, and functional electrical stimulation (FES) may all play a role.10 The dawning of the 21st century saw the design of various interfaces allowing computer influence on neuronal function. These human-machine interfaces present the tantalizing possibility of a decrease in disabilities and an increase in functional independence.11 At a significant cost to the patient, neuroprosthetics that utilize electrical stimulation to nerves and muscular motor units can now be purchased. These may enable certain movements that the uninjured, healthy individual may take for granted, such as emptying of the bladder.11 Devices for functional neuromuscular stimulation (FNS), which is also referred to as FES, have been developed to promote functional movements of otherwise paralyzed muscles.11 These advances, however, have surfaced in the face of various roadblocks, involving disputes with regulatory agencies over efficacy and safety issues, cost-benefit analysis, and limited markets.11 Table 15.1 Spinal Cord Injury Variations
 SCI Financial Costs
SCI Financial Costs
 The Role of Modern Technology
The Role of Modern Technology
| C1-C3 tetraplegia | • Long-term mechanical ventilatory support |
| • Head, neck, possibly shoulder mobility | |
| • Dependent on others for rest of mobility and self-care | |
| • Swallowing and phonation preserved | |
| C1-C4 tetraplegia | • Same as above, except injury at C4 level generally does not require mechanical ventilation |
| • Communicate via assistive technology (e.g., environmental control units) | |
| C5 tetraplegia | • Functional elbow flexion |
| • Eat and groom independently with assistive devices | |
| • Require assistance for most self-care | |
| C6 tetraplegia | • Addition of functional wrist extension and passive thumb adduction on index finger during wrist extension |
| • Functional independence with assistive devices for feeding, grooming, bathing, bed mobility | |
| • Can assist with bladder and bowel program | |
| • Manual or power wheelchair use | |
| C7 tetraplegia | • Highest level of injury where one can still live independently |
| • Functional independence in most things requiring upper body, and independence with use of assistive devices for lower extremities | |
| • Can write, type, answer phone, use computer | |
| C8 tetraplegia | • Functional finger flexion resulting in increased grasp |
| • Functionally independent | |
| • Can drive in specialized car with hand controls | |
| Thoracic paraplegia | • Innervation and function of all upper extremities |
| • Functionally independent at wheelchair level | |
| • Can also drive specialized car | |
| Lumbar paraplegia | • Functionally independent for all mobility, self-care, bladder and bowel skills |
| • Like thoracic, may need advanced wheelchair training | |
| • Drive specialized car |
In a study by Jack Edwards, 470 individuals with SCIs were enrolled in upright mobility programs, which involved the use of a reciprocal gait orthosis (RGO). These individuals could walk distances of over 300 m at speeds of 0.2 to 0.5 m/s. In addition, a distance of 0.6 km could be achieved without having to sit down. Incidence of pain, spasms, and urinary and respiratory tract infections were all decreased.12
Michael Keith examined the results following implantation of the Freehand (NeuroControl Corp., Cleveland, Ohio) neuroprosthesis, which attempts to re-create hand motion in tetraplegics. At the time of the study, approximately 200 neuroprosthetics had been implanted. Compared with their preoperative state, patient independence was improved by an average of 85%.12
Cotler et al13 assessed the beneficial role of orthotics used in patients with closed cervical spine dislocations. Two populations were examined: patients using orthotics with previous nonoperative treatment, and those patients using orthotics with previous operative treatment. Better outcomes were seen in those treated operatively at an early time. Approximately 64% of those treated nonoperatively sustained a redisplacement of their dislocation. The study showed an average financial savings of $18,407 in those treated operatively.
 Spinal Cord Injury Studies
Spinal Cord Injury Studies
Several studies examined the socioeconomic costs related to SCI. Dryden et al14 followed 233 patients suffering an SCI in Canada for 6 years from the date of injury. Patients were matched with a group of 1165 randomly selected patients from the general population for age, gender, and region of residence and were followed for 6 years. Costs were calculated from central databases and included health care use, hospitalizations, physician contacts, long-term care admissions, home health care services, and secondary complications. Results demonstrated that SCI patients were rehospitalized 2.6 times more often, and when hospitalized the SCI patients required an average of 3.3 more days. SCI patients contacted physicians 2.7 more times and required 30 times more hours on home health care. Of the medical complications suffered by SCI patients, almost 48% suffered urinary tract infections, 34% pneumonia, 28% depression, and 20% decubitus ulcers (Table 15.2). The study demonstrated the magnitude of long-term posttraumatic secondary care often required by SCI patients and its associated costs.
In 2003 a large systematic review was performed analyzing the costs and effectiveness of surgical spinal fixation for SCI and delayed versus immediate surgical referral to an SCI unit.15 Sixty-eight studies on spinal fixation versus no spinal fixation were reviewed and suggested benefits of spinal fixation surgery. Of the 68 studies, only four were performed in specific spinal injury units, and in these centers there were no benefits demonstrated with spinal fixation. There were 28 retrospective observational studies reviewed on the benefits of referral to a spinal injury unit, which suggested that referral to a spinal injury unit did improve overall neurologic outcomes. Authors went on to recommend that primary research involving audits of selected hospital records be commissioned and published. In addition, future research should include full economic evaluations alongside randomized controlled studies, which can then consider the costs of implementing certain treatments in SCI.
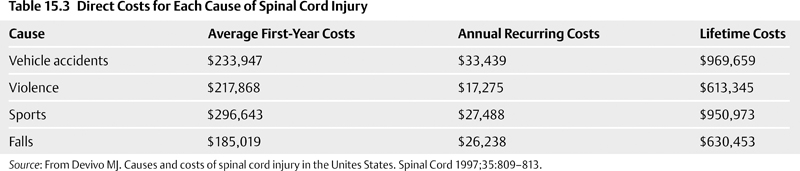
DeVivo6 performed a cross-sectional multicenter study to estimate the direct costs of each cause of spinal cord injury. The purpose was to compare random samples of 227 new injuries and 508 patients postinjury ranging from 2 to 16 years. Prospective data collected for 1 year included emergency medical services, hospitalizations, home health care, equipment, supplies, medications, environmental modifications, physician and outpatient services, nursing homes, household assistance, vocational rehabilitation, and miscellaneous items. The injury types were categorized and first-year costs compared along with recurring annual costs and projected lifetime costs. Motor vehicle accidents averaged $233,947 (annual recurrence $33,439, lifetime $969,659), violence $217,868 ($17,275, $613,345), sports $296,643 ($27,488, $950,973), and falls $185,019 ($26,238, $630,453). The leading cause of SCI in sports is diving (66%) (Table 15.3). Males comprise 82% of SCI patients, and 57% are in the age range of 16 to 30 years at the time of injury.
The direct costs were then calculated based on the approximately 11,000 cases of SCI per year, 2% discount rate-a discount function f(t) specifying the present value of a unit payment time t in the future-survival data from the National Spinal Cord Injury Statistical Center, and the incidence of each type of SCI.2 Thus, motor vehicle accidents are 36% of all SCIs and cost the United States approximately $3.48 billion; violence 30%, $1.81 billion; falls 20%, $1.28 billion; and sports 7.0%, $694 million. The study demonstrated that total direct costs to the United States would approximate $7.7 billion based on 1995 income. These costs were not isolated to the health care industry. For example, because motor vehicle accidents are the leading cause of SCI in patients, the automotive industry remains very involved in researching ways to better safeguard vehicles, in the hopes of minimizing SCI to their occupants. Everything from vehicle rollover to the more commonly seen accident types resulting in SCI have been studied.16
Table 15.2 Dryden Study of Spinal Cord Injury Patients Versus Non-Spinal Cord Injury Patients
| SCI patient characteristics | • Rehospitalized 2.6 times more often |
| • Required a length of stay averaging 3.3 days longer | |
| • Contacted physicians 2.7 more times | |
| • Required 30 times more hours on home health care | |
| Medical complications suffered by SCI patients | • 48% urinary tract infections |
| • 34% pneumonia | |
| • 28% depression | |
| • 20% decubitus ulcers |
Regarding the role of violence in SCI, gunshot wounds are currently the second leading cause of spinal cord injury in the United States Concomitant injuries or complications accompanying gunshot wounds often increase patient morbidity as well. McKinley et al17 studied a patient base of 217, over a 5-year period, admitted to a hospital due to traumatic SCI. Of these hospital admissions, a total of 49 cases involved gunshot-related events. Common medical complications accompanying these cases included pain (54%), infections (40%), pneumothorax (24%), nonspinal fractures (22%), colonic perforation (17%), cerebrospinal fluid leak (10%), and retroperitoneal hematoma (10%) (Table 15.4). This study revealed that complete SCI and paraplegia were the most common injury types in gunshot-related SCI. It is also important to note that although patients with these injuries had lengths of hospital stays similar to nonviolent SCI, there seemed to be a specific population base more at risk for the violence-related SCI, that being a younger, non-Caucasian, unmarried, and unemployed adult population.
More recent studies have focused on direct and indirect costs. Dryden et al18 in 2005 focused on the direct costs in Canada of SCI attributed to trauma. Patients were classified as complete SCI or incomplete SCI. Data were compared from centralized health databases for first-year costs and subsequent annual costs for 5 years. These costs included hospitalizations, physician services, home care, and long-term care. First-year costs for complete SCI were $121,600 and for incomplete SCI were $42,100. Subsequent annual costs for 5 years averaged $5400 for complete and $2800 for incomplete (Table 15.5). As expected, the study demonstrated that complete SCI patients accrue greater total costs, and the first-year costs for taking care of complete and incomplete SCI patients is substantial.
In comparison to direct costs of care in SCI patients data from the United States in 2004, high tetraplegics’ first-year costs were estimated to be $683,000 and each subsequent year $122,334; for low tetraplegics, these costs are $441,025 and $50,110; for paraplegics, $249,549 and $25,934; and for incompletes, $201,273 and $14,106. These drastic differences are due to the bundling of so-called direct costs. The direct costs in this study included hospitalizations, physician services, home health care attendants, durable medical equipment, home modifications, medications, medical supplies, and transportation (Table 15.5).2
 Direct Psychological and Sociologic Effects
Direct Psychological and Sociologic Effects
To date, there are numerous studies demonstrating that SCI patients suffer higher lifetime unemployment rates, significant income losses, reduced life expectancy, long-term health care requirements and costs, significant pain and suffering, reduced likelihood to marry or remain married, and an alarmingly high suicide rate at almost five times greater than that of the general United States population.19 The suicide rate does not significantly change beyond the fifth year after injury. DeVivo19 found that suicide was the leading cause of death in SCI for complete paraplegics and the second leading cause for incomplete paraplegics. Self-inflicted gunshot was the most common route chosen for suicide (Table 15.6).
Employment rates on SCI patients, as determined by the National Spinal Cord Injury Association, are 61% at the time of injury and 13.6% by the end of the first year after injury.2 Due to advances in SCI research, an increasing number of SCI patients are returning to work, with 30% of quadriplegics and 40% of paraplegics eventually returning to work. Overall unemployment averages approximately 50% for SCI patients in the 20 years following the injury.
Table 15.4 Complications Associated with Gunshot Wound-Induced Spinal Cord Injury
| Pain | 54% |
| Infections | 40% |
| Pneumothorax | 24% |
| Nonspinal fractures | 22% |
| Colonic perforation | 17% |
| Cerebrospinal fluid leak | 10% |
| Retroperitoneal hematoma | 10% |
Table 15.5 Comparing Costs of Complete Versus Incomplete Spinal Cord Injury
| Dryden et al18 Study: Canada 2005 | ||
| First-Year Costs | Subsequent 5-Year Annual Costs | |
| Complete SCI | $121,600 | $5400 |
| Incomplete SCI | $42,100 | $2800 |
| Costs include: | Hospitalizations, physician services, home care, and long-term care | |
| NSCISC Statistics2: United States 2006 | ||
| First-Year Costs | Subsequent Annual Costs | |
| High tetraplegics | $683,000 | $122,334 |
| Low tetraplegics | $441,025 | $50,110 |
| Paraplegia | $249,549 | $25,934 |
| Incomplete SCI | $201,273 | $14,106 |
| Costs include: | Hospitalizations, physician services, home health care attendants, durable medical equipment, home modifications, medications, medical supplies, and transportation | |
Abbreviation: NSCISC, National Spinal Cord Injury Statistical Center.
Among other social effects of SCI is sexual dysfunction. The high incidence of erectile dysfunction following traumatic SCI can have a considerable effect on the quality of life of patients and their significant other. There are treatment options available for these patients, including sildenafil administration, intracavernous injections of papaverine/alprostadil (Caverject), alprostadil/papaverine/phentolamine (“triple mix”), transurethral suppository medicated urethral system for erections (MUSE), surgically implanted prosthetic devices, and vacuum erection devices.20 Cost-effective analysis has shown that sildenafil was the most economically sensible treatment when compared with surgically implanted prosthetic devices, MUSE, and Caverject.20 Basic statistical studies have also demonstrated that SCI patients who are single at the time of injury are more likely to remain single than an age-matched non-SCI person. In addition, those SCI patients who are married at the time of injury have a divorce rate of almost 20% in the first 5 years postinjury, while the age-matched comparison calculations found a rate of 11% for a non-SCI person.2
Spinal cord injury patients experience continuing medical problems requiring lifetime medical care and medical expenses. The average SCI patient spends 79 days in the hospital after the injury, and first-year costs and added living expenses directly attributable to SCI vary substantially by the severity of the injury.
Table 15.6 Direct Psychological and Socioeconomic Effects of Spinal Cord Injury
| Psychological | • Depression |
| • Reduced life expectancy | |
| • Significant pain and suffering | |
| • Reduced likelihood to marry or remain married | |
| • Higher suicide rate* | |
| Socioeconomic | • Higher lifetime unemployment rates |
| • Significant income losses | |
| • Long-term health care requirements and costs |
* It is important to note that the suicide rate for SCI patients was five times that of the general population, with gunshot being the most common route.
 Indirect Psychological and Sociologic Effects
Indirect Psychological and Sociologic Effects
Costs of SCI impacts a larger portion of the population than just the patients themselves and are not always reflected in dollars. Weitzenkamp et al21 performed an interesting study on the social impact to the spouse of the SCI patient. Social demographics, health concerns, depression tests, perceived stress scales, and life satisfaction indices were analyzed. Spouses of SCI patients (n = 124) were tested, all of whom had been with an SCI patient for 23 or more years. Interestingly, spouses of SCI patients had a more depressive affect (p < .001) than did their partners with SCI. There were no differences in perceived stress scales between the spouses and SCI patients. However, when spouses were categorized into caregiving and noncaregiving, the caregiving spouses demonstrated significantly more stress than their SCI partners and noncaregiving spouses (p = .005). Conclusions were that spouses of SCI patients who perform a caregiving role suffer significantly more stress and depression than their partners with SCI or the spouses who are not caregivers.19
Table 15.7 Common Psychological Effects of Spinal Cord Injury: The “4 D’s”
| 1. Depression | 25 to 45% of SCI patients suffer from some form of depression |
| 2. Dependency | Increased dependence on others for everyday tasks and self-care |
| 3. Drug addiction | Increased use of narcotics and alcohol in SCI patients |
| 4. Divorce | 20% divorce rate of SCI patients compared with 11% for non-SCI individuals |
Christian22 discussed the most common psychological issues that are seen in those suffering from SCIs. In his book, he referred to the work of Joyce Fichtenbaum, PhD, and Steven Kirschblum, MD, and their identification of the “4 D’s” (Table 15.7): depression, dependency, drug addiction, and divorce; 25 to 45% of those suffering from SCI experience a certain level of depression following their injury. This can have several manifestations, from loss of appetite or decreased attention, to suicidal tendencies. An increased dependency on the health care team is frequently observed. It is very important that patients learn to maximize all of their functional capabilities before giving in to complete dependence on others. Increases in drug and alcohol abuse have also been seen. This tendency should be addressed as soon as possible.
 Long-Term Disability Costs and Longevity
Long-Term Disability Costs and Longevity
When discussing life expectancy in SCI, one must consider the five types of SCI: ventilator dependent, high tetraplegic, low tetraplegic, paraplegic, and incomplete. In general, the least severe forms of SCI have a life span decrease of only approximately 10%, varying to almost a 70% reduction in life expectancy for the most severe form (ventilator dependent) of SCI.2
| Ages | Risk Ratio of Death Due to Respiratory Disease |
|---|---|
| 31-45 | 4.87 times greater risk |
| 46-60 | 19.04 times greater risk |
| 61 and older | 45.98 times greater risk |
Diseases of the respiratory system were the leading cause of death (71% of these were cases of pneumonia). Supporting evidence can be seen in a study by Frankel et al,23 showing that the cause of death in the period 1973 to 1990 in a sample population of 226 patients was pneumonia, influenza, or other respiratory diseases in 76 patients (34%). The study also showed that SCI patients between the ages of 31 and 45 were 4.87 times more likely to die from respiratory problems than those under the age of 30. This risk ratio quadruples to 19.04 for those between the ages of 46 and 60, and further increases to 45.98 for those 61 or older, which stands as the group most vulnerable to death from respiratory disease (Table 15.8). These infections arise mainly due to weakened respiratory muscles and difficulty removing secretions, which then tend to build up in the lungs, predisposing an individual with SCI to subsequent infection.22 The diaphragm is the most important muscle involved in respiration and is innervated by the phrenic nerve (C3-C5). The abdominal muscles, which have T6 and L1 innervation, can also become important in the breathing process, especially in forced expiration and inspiration, or if there is phrenic nerve dysfunction.22 High and midlevel cervical spinal cord injuries can result in paralysis of the diaphragm and a subsequent increased longevity of mechanical ventilator dependence. Proper ventilator management is necessary and involves the constant monitoring of inspiratory and expiratory muscles, aspiration, clearing of secretions, potential lung parenchyma injury, bronchoconstriction, and nutrition. Phrenic nerve conduction studies can be made to assess the possibility of nerve recovery.24
Heart disease ranked as the second most common cause of death in SCI; however, these were often unexplained heart attacks (55%). Although some recent studies have actually shown that for long-term SCI, morbidity and mortality from causes related to the cardiovascular system, particularly coronary artery disease, have surpassed those from renal and pulmonary conditions, most authors still consider it the second leading cause of death.25 Underlying risk factors in the SCI patient include a sedentary lifestyle and decreased physical activity, hyperlipidemia, obesity, and diabetes (Table 15.9). Furthermore, the disturbance of normal autonomic cardiovascular control seen in SCI patients puts these individuals at risk.25 These effects are more commonly seen in injuries occurring at or above the T6 level of the spinal cord.22 Abnormalities are seen in blood pressure, heart rate variability, arrhythmias, and a decreased cardiovascular response to exercise, limiting one’s ability to perform physical activity. Hypotension is commonly seen in SCI patients as the combination of lower leg paralysis and gravity results in blood pooling below the waist, thus limiting venous return to the heart. In the attempt to move, such as getting out of a wheelchair, dizziness due to orthostatic hypotension is a common side effect.22 Tetraplegics experience a 16% higher risk of all cardiovascular disease, whereas paraplegia corresponds with a 70% higher risk of developing coronary artery disease. All the factors present in Table 15.2 play a role in determining the care and treatment of SCI patients, which then determines the cost of treatment for each individual. With these factors present, these patients can no longer be treated strictly as SCI patients.
Table 15.9 Risk Factors of Cardiovascular Disease in Spinal Cord Injury Patients
| Low HDL, high total cholesterol, high LDL | Blood pressure abnormalities |
| High C-reactive protein | Deep vein thrombosis, thromboembolic events |
| High prevalence of obesity | Rhythm disturbances (bradyarrhythmias, decrease in heart rate variability) |
| High rate of smoking | Diabetes, metabolic syndrome |
| Sedentary lifestyle | Decrease in cardiovascular response to exercise |
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
The third leading cause of death was bacterial infection and parasitic diseases. Most of these patients had septicemia (93%) and usually had decubitus ulcers (discussed in more detail later in the chapter) and urinary tract or respiratory infections. Urinary tract infections are a common development in those with SCI because the bladder may not be emptying completely, or simply may not be emptying frequently enough. The bladder itself then essentially becomes a prime location for infection. It is also not uncommon to resort to the use of catheters to drain the bladder, which always presents the risk of introducing infection during insertion. It has also been shown that untreated urinary infections can then predispose the patient to other adverse health problems, such as pyelonephritis, septicemia, and kidney stones. Education provided to the patient and family pertaining to this risk of infection and the importance of self-monitoring is very important in the prevention of these complications.26 Hypertensive heart disease and suicide competed for the fourth and fifth leading causes of death in multiple studies.
The value of a life is an actively researched and highly controversial area in the socioeconomic literature, and a survey in 1993 concluded that the results cluster in the $3 million to $7 million range.27 Federal agencies are currently required to use $5.8 million as the value of life.28 The value per year of life remaining averages $180,000 in 1986 dollars.29 Moore and Viscusi’s29 results, when combined with three other studies, provide one estimate of the value of reduced life expectancy due to SCI.12 For example, a low tetraplegic SCI incurred by a 40-year-old (who survives the first year after injury) would reduce life expectancy by 14 years, and at $180,000 per year, the value of the lost years is $2,520,000 in 1986 dollars. Recent research by the NSCISC has found that the cumulative 20-year survival rate for patients with spinal cord injury was approximately 71% (Table 15.10).2
Unemployment leads to elevations in indirect costs, which include lost wages, fringe benefits, and productivity. The average SCI patient loses $57,000 annually, which by estimation of the total number of SCI patients and annual losses equals approximately $16 billion to $26 billion per year.2
 Initial Hospitalization Costs
Initial Hospitalization Costs
Mean days hospitalized in the SCI care system’s acute and rehab units are greater for persons with tetraplegia than for those with paraplegia (Table 15.11). In most years, the difference in acute care length of stay between persons with tetraplegia and those with paraplegia is relatively small, whereas differences in rehabilitation length of stay are substantial. Mean days hospitalized in the acute care unit are usually greater for patients with neurologically complete cervical injuries than for patients with neurologically incomplete cervical injuries. Mean days hospitalized in the system’s acute care unit for persons with neurologically complete tetraplegia ranged from 46 in 1982 to 16 in 1997, whereas for those with neurologically incomplete paraplegia, the comparable range was from 29 days in 1973 and 1982 to 11 days in 1999. Mean days hospitalized in the rehab unit are greatest for patients with neurologically complete injuries. Mean days hospitalized in the system’s rehab unit for persons with neurologically complete tetraplegia ranged from 165 in 1975 to 59 in 2002, and for those with neurologically incomplete paraplegia, the comparable range was from 90 days in 1975 to 30 days in 2001.2
Table 15.10 The “Value of Life”
| • A 1993 survey concluded the value of life is $3 million to $7 million |
| • Federal agencies are currently required to use $5.8 million for the value of life |
| • The value per year of life remaining averages $180,000 in 1986 dollars |
| • A low tetraplegic SCI incurred by a 40-year-old who survives the first year after injury would reduce life expectancy by 14 years, and at $180,000 per year, the value of the lost years is $2,520,000 in 1986 dollars |
| • Recent 20-year survival rate for SCI patients has reached 71% |
Table 15.11 Mean Days Hospitalized in Spinal Cord Injury Care System
| Acute care facility | |
| Neurologically complete tetraplegia | • 1982: 46 days |
| • 1997: 16 days | |
| Neurologically incomplete paraplegia | • 1973 and 1982: 29 days |
| • 1999: 11 days | |
| Rehab facility | |
| Neurologically complete tetraplegia | • 1975: 165 days |
| • 2002: 59 days | |
| Neurologically incomplete paraplegia | • 1975: 90 days |
| • 2001: 30 days | |
In constant 2003 dollars, mean total system charges (Table 15.12) increased from $150,328 during 1973 and 1974 to $236,136 in 1991 and 1992. This increase most likely reflects the trend toward improved survival of more severely injured persons at the scene of the injury who subsequently require greater intensity of service (such as mechanical ventilation) despite declining rehabilitation lengths of stay. Since 1992, mean total system charges decreased to only $206,176 in 2002 but increased again to $254,161 in 2003.2
Table 15.12 Total Mean Charges for Care (2003 dollars)
| Year | Total Mean Charges |
|---|---|
| 1973-1974 | $150,328 |
| 1991-1992 | $236,136 |
| 2002 | $206,176 |
| 2003 | $254,161 |
 Post-Spinal Cord Injury Complications/Rehospitalizations
Post-Spinal Cord Injury Complications/Rehospitalizations
The most frequent complication is pressure (decubitus) ulcers observed during the annual examination, beginning at 15% in the first postinjury year and steadily increasing thereafter. Due to immobility and the fact that these patients have no feeling of pressure or pain below the level of injury, they often fail to shift their weight to relieve the pressure. In addition, skin care, irritation, and nutritional deficiency can play an integral role in the development of these pressure sores. Once again, education and information access and delivery are in the forefront for prevention. Although they may appear superficial, untreated sores can progress to a state of massive infection and even to necrosis of the skin and underlying tissues. This infection can ultimately involve the bone.26 Even though aggressive early intervention, followed by discharge to a rehabilitation facility, is ideal, the average stay prior to transfer was 32.7 days.8 In a study by Fielingsdorf and Dunn,8 a 2-week goal for transfer was established, and only 40% of the SCI patients met this goal. This followed significant delays in admission due to the distances involved and limited bed availability; 50% of the patients were admitted on either the day of injury or the day following, whereas 67% were admitted within 2 days of the date of injury. These delays have a significant impact on morbidity, as seen by the incidence rates of pressure sores of 11% upon admission to the unit. Another 11% then develop these sores during their stay in the rehab facility. It is important that adjustments be made to ensure resource allocation to this area to reduce pressure ulcer incidence, or else it will remain a significant problem in prolonging hospital stay and adding greatly to the cost of care.
The next most common complication was pneumonia, which ranged from 2.5 to 3.9% over time. For those patients rehospitalized, the average length of stay was relatively constant over time (26 days in the first postinjury year and 20 days in the 25th year). Diseases of the genitourinary system were the leading cause of rehospitalization during postinjury years 1, 10, 15, 25, and 30, whereas diseases of the skin were the most common cause of rehospitalization during postinjury years 5 and 20. Circulatory, respiratory, digestive, and musculoskeletal diseases and conditions were also relatively common causes of rehospitalization.2
 Past, Present, and Future: Moving Forward
Past, Present, and Future: Moving Forward
In 1970, the first regional SCI system was established in Phoenix, Arizona.5 By the early 1990s, a total of 19 centers were receiving government funding. Two models of SCIrehabilitation programs were eventually established: free-standing rehab clinics and rehab units within acute care facilities. Although the latter type provides the opportunity of a continuum of care, from emergency medical services to acute inpatient rehabilitation, very few clinics have used this continuum.5 Thus, they have not seen the many benefits that can result in establishing an SCI program that provides acute care, rehab, and therapeutic services all at the same location. These benefits include, but are not limited to, fewer postinjury complications (e.g., decubitus ulcers) for those admitted less than 24 hours from injury, decreased costs of acute care for patients admitted within this 24-hour window (a reported $5000 savings in 1992), and shorter rehab length of stays.5 However, this type of clinic may clash with the evolving SCI program structure that has deviated from the fee-for-service reimbursement system to a Medicare-based prospective payment system.
The area of SCI remains a highly attractive field for research due to an overwhelming clinical need for prevention and effective therapy.30 Previous clinical trials need to be examined to reveal and correct any inadequacies. The incorporation of new trial designs discovered in other fields, such as cancer research, that are applicable to SCI studies can also be examined.30 Continued improvements in SCI clinical trials, such as the use of randomized prospective controlled trials, adoption of a uniform clinical grading system, and development of other dependable outcome measures, facilitate conducting better, more efficient trials. By way of these changes, possible improvements can be made in the quality of care and cost-effectiveness of treatment plans for SCI patients.
With the exception of the Veterans Affairs system, most SCI programs involve long-term care at outpatient clinics, following discharge from an acute care facility. Follow-up care involves annual checkups, but little effort is made to provide primary care services.5 It should be obvious that such a fragmented system results in clinical outcomes that are less than ideal, at a much greater overall cost. If the future of SCI care remains in outpatient therapy clinics, then primary care services must be provided, allowing both the initial access to rehab services and a study of the long-term health care needs of patients within this system.
References
2. The National Spinal Cord Injury Statistical Center, University of Alabama at Birmingham, 2006
3. American Association of Neurological Surgeons. Spinal cord injury. http://www.neurosurgerytoday.org/what/patient_e/spinal.asp; 2005
9. McKinley W, Silver TM, Santos KG, Pai AB. Functional outcomes per level of spinal cord injury. eMedicine (online from WebMD): http://www.emedicine.com/pmr/topic183.htm#sectionapproximately c1-c4,_or_high,_tetraplegia; 2006
19. DeVivo MJ. Suicide following spinal cord injury. Paraplegia 1991;29:620–627
24. Strakowski JA, Pease WS, Johnson EW. Phrenic nerve stimulation in the evaluation of ventilator-dependent individuals with C4- and C5-level spinal cord injury. Am J Phys Med Rehabil 2007;86: 153–157
27. Viscusi WK. The value of risks to life and health. J Econ Lit 1993;31:1912–1946
28. Peterson CH. Business and Government. 4th ed. New York: Harper & Row; 1996
< div class='tao-gold-member'>




