Chapter 67 Severe head injury
Despite improvements in resuscitation and vital organ support, the management of patients with traumatic brain injury in the intensive care unit (ICU) presents a challenge to all members of the critical care team. As head injury is associated with a high mortality and morbidity, the benefits of intensive treatment and care may not become apparent until months or years later during rehabilitation after injury.
EPIDEMIOLOGY
AETIOLOGY
Vehicular trauma, industrial accidents, falls and assaults account for the majority of head injury, with marked variations in patterns of injury across the world. For example, in Australasia, the incidence of head injury due to vehicular trauma is decreasing due to the success of preventive strategies such as restraint devices, speed control and stricter drink-driving legislation.1
PATHOPHYSIOLOGY
Brain injury is a heterogenous pathophysiological process. It encompasses a spectrum of injury that includes the degree of brain damage at the time of injury (primary injury) in addition to insults that occur during the post-injury phase (secondary injury). These processes are depicted in Figure 67.1.
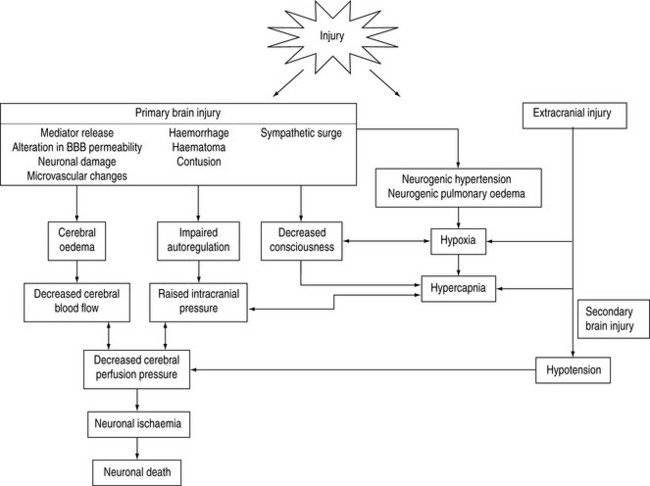
SECONDARY BRAIN INJURY
Secondary brain insults are characterised by a reduction in cerebral substrate utilisation, particularly oxygen (Table 67.1). Of these insults, hypotension (defined as a systolic blood pressure of < 90 mmHg), hypoxia (oxygen saturation < 90% or PaO2 < 50 mmHg), hypoglycaemia, hyperpyrexia (temperature > 39°C) and prolonged hypocapnia (PaCO2 < 30 mmHg) have been shown to independently worsen survival following traumatic brain injury.
Table 67.1 Secondary brain insults following traumatic brain injury that are associated with increased morbidity and mortality
| Systemic | Intracranial |
|---|---|
| Hypoxia | Seizure |
| Hypotension | Delayed haematoma |
| Hypocapnia | Subarachnoid haemorrhage |
| Hypercapnia | Vasospasm |
| Hyperthermia | Hydrocephalus |
| Hypoglycaemia | Neuroinfection |
| Hyperglycaemia | |
| Hyponatraemia | |
| Hypernatraemia | |
| Hyperosmolality | |
| Infection |
INTRACRANIAL INFLAMMATION
Traumatic brain injury invokes an inflammatory response characterised by the release of cytokines, freeradicals, excitatory amino acids and other mediators. The consequence of this response is disruption and alteration in the permeability of the blood–brain barrier, glial swelling and alterations in regional and global cerebral blood flow. The extent of this inflammatory process is an important determinant of intracranial pressure that may persist for some time following injury. Furthermore, alteration in blood–brain permeability may render the cerebral circulation susceptible to the effects of drugs that do not normally cross, such as osmotic diuretics and exogenous catecholamines.
CEREBRAL BLOOD FLOW AND AUTOREGULATION
Normally, cerebral blood flow is maintained at a constant rate in the presence of changing perfusion pressures by myogenic and metabolic autoregulation. These homeostatic mechanisms are impaired following head injury due to neuronal damage and intracranial inflammation. Distinct patterns of cerebral blood flow have been described following head injury that have direct clinical relevance with regard to management2 (Figure 67.2).
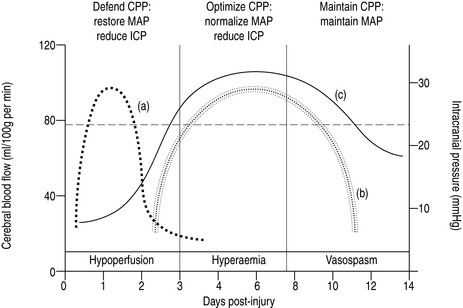
THE HYPOPERFUSION PHASE
In order to maintain cerebral perfusion, systemic blood pressure must be maintained during this phase so that cerebral perfusion pressure (defined as the difference between mean arterial pressure and intracranial pressure) is maintained between 60 and 70 mmHg.3
THE HYPERAEMIC PHASE
This hyperaemic phase may persist for up to 7–10 days post injury and occurs in 25–30% patients. As there is restoration or increased cerebral blood flow during this phase, a range of cerebral perfusion pressure is recommended (50–70 mmHg).4
THE VASOSPASTIC PHASE
In a small cohort of patients (10–15%), particularly those with severe primary and secondary injuries or those with significant traumatic subarachnoid haemorrhage, a vasospastic phase characterised by typical cerebral blood flow patterns may persist. This phase represents a complex of cerebral hypoperfusion due to arterial vasospasm, posttraumatic hypometabolism and impaired autoregulation.5
RESUSCITATION
INITIAL ASSESSMENT
The resuscitation of head-injured patients should follow the principles outlined in the Advanced Trauma Life Support (ATLS®) guidelines for the early management of severe trauma.6
With respect to head-injured patients, the following principles in the initial assessment apply.7,8
BREATHING (= VENTILATION)
Empirical hyperventilation during initial resuscitation is not indicated until adequate oxygenation, haemodynamic stability and urgent computed tomography have been achieved.9
CIRCULATION (= CONTROL OF SHOCK)
Prompt restoration of circulating blood volume and restoration of a euvolaemic state is critical.10
An emerging body of evidence recommends the use of crystalloids, specifically normal saline, for fluid resuscitation of patients with traumatic brain injury. The use of albumin for fluid resuscitation is associated with increased mortality and should be avoided.11 Hypertonic saline may have a role as a small-volume resuscitation fluid that is useful in expanding intravascular volume, with additional beneficial effects on cerebral blood flow and reduction of cerebral oedema,12 although there is no evidence of reduced mortality when used in the prehospital period.13
Inotropes, such as adrenaline (epinephrine) or noradrenaline (norepinephrine), or vasopressors such as phenylephrine or metaraminol, may be used to defend blood pressure once correction of hypovolaemia is underway or achieved.4 This may be necessary if sedatives or narcotics are coadministered.
The use of military antishock trousers (MAST suit) in traumatic brain injury is not recommended.
DISABILITY (= NEUROLOGICAL ASSESSMENT)
Level of consciousness
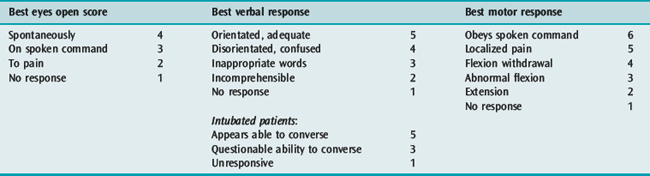
The Glasgow Coma Scale (GCS) has an established place in the management of traumatic brain injury and is the most widely accepted and understood scale.14 Whilst originally described as a prognostic index, it provides an overall assessment of neurological function, derived from three parameters: eye opening, verbal response and motor response (Table 67.2).
Table 67.2 The Glasgow Coma Scale.14 The best response following non-surgical resuscitation is scored
Pupillary responses
In the absence of traumatic mydriasis, abnormalities of pupil size and reactivity may indicate compression of the third cranial nerve, suggesting raised intracranial pressure or impending herniation, particularly when associated with lateralising motor signs and depressed consciousness
Papilloedema is uncommon in the acute phase of head injuries.
SECONDARY SURVEY
Once the initial assessment is complete and resuscitation underway, a thorough secondary survey adopting a ‘top-to-toe’ approach is mandatory. This is outlined in the ATLS® approach to the traumatised patient.6
BRAIN-SPECIFIC RESUSCITATION
HYPERVENTILATION
Ventilation-induced reductions in PaCO2 result in marked reductions in cerebral blood flow and consequently in intracranial pressure. However, as cerebral blood flow may be reduced during the initial period following injury, further reductions in cerebral perfusion will result if hyperventilation is used during this phase (Figure 67.2).
However, hyperventilation remains a potent non-surgical clinical tool of reducing intracranial pressure. In the resuscitated head-injured patient with unequivocal clinical signs of raised intracranial pressure or impending tentorial herniation (pupillary dilatation, lateralising signs or a witnessed neurological deterioration), hyperventilation is an option.Reductions of PaCO2 to levels ≤30 mmHg (4 kPa) may be therefore considered prior to urgent imaging or surgery for evacuation of a mass lesion.9
OSMOTHERAPY
Given the high risk with minimal benefit during resuscitation, the routine use of mannitol is not recommended in the absence of raised intracranial pressure and in patients where cerebral blood flow is compromised.15
Hypertonic saline (3% solution) exerts similar osmotic plasma expanding effects to mannitol. These solutions do not exert an osmolal gap so that serum sodium reflects serum osmolality allowing easier titration. These solutions have been advocated as ‘small-volume resuscitation fluids’ that may be very effective in restoring systemic and cerebral perfusion in the acute phase following injury. In addition to reducing intracranial pressure, these solutions would appear to be superior to mannitol for resuscitation.16
IMAGING
X-RAYS
All head-injured patients receive the routine ‘trauma series’ of X-rays, namely chest, pelvis and cervical spine (lateral, anteroposterior and peg views), although the last may be superseded by high resolution CT scan of the entire cervical spine.17
COMPUTED TOMOGRAPHY (CT SCAN)
The following patients should undergo CT head scan following traumatic brain injury:
Technological advances in imaging now enable quick, high resolution digital images of the brain parenchyma and bony compartments. The most important role of CT scanning is prompt detection of mass lesion such as extradural or subdural haematomas. Thereafter, the degree of brain injury may be quantified by radiological criteria (Table 67.3 and Figure 67.3a).18
Table 67.3 Classification of CT scan appearance following traumatic brain injury.16 Examples are shown in Figure 67.3a
| Category | Definition |
|---|---|
| Diffuse injury (DI) I | No visible intracranial pathology seen on CT scan |
| DI II (diffuse injury) | Cisterns are present with midline shift 0–5 mm and/or Lesion densities present No high or mixed density > 25 mm May include bony fragments and foreign bodies |
| DI III (swelling) | Cisterns are compressed or absent with midline shift 0–5 mm No high or mixed density > 25 mm |
| DI IV (shift) | Midline shift > 5 mm No high or mixed density > 25 mm |
| Evacuated mass lesion | Any lesion surgically evacuated |
| Non-evacuated mass lesion | High or mixed density lesion > 25 mm, not surgically evacuated |
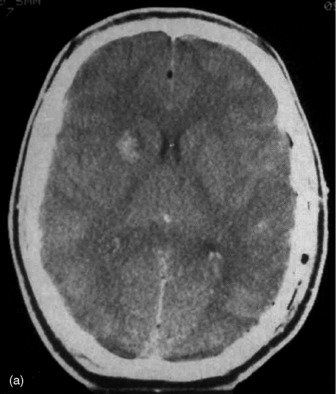
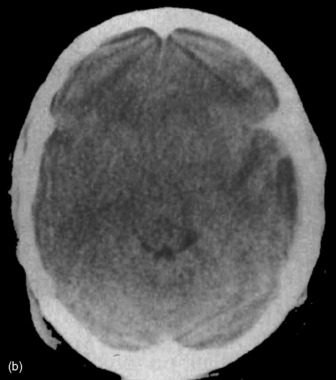
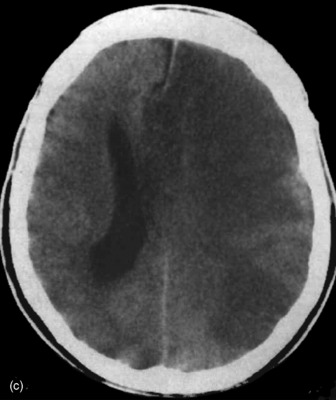
Figure 67.3a Computed tomographic classification of diffuse axonal injury (Table 67.3).33 Panel (a) Diffuse injury II; Panel (b) Diffuse injury III; Panel (c) Diffuse injury IV.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


