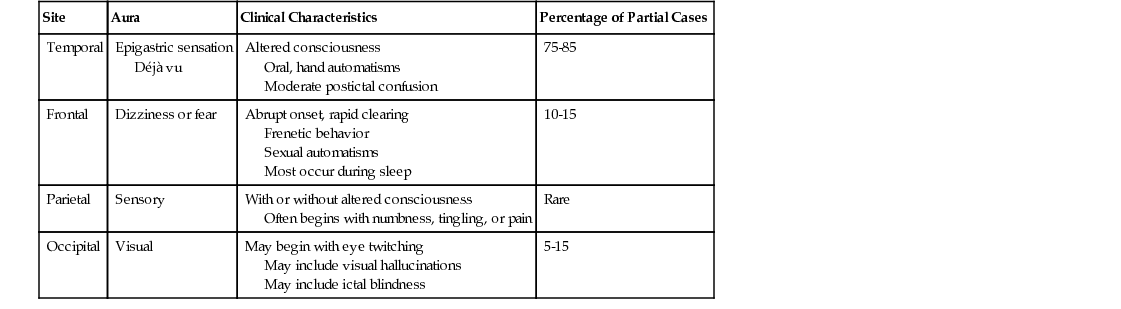
Karen L. Secore Epilepsy, a syndrome of recurrent (unprovoked) seizures, is a common neurologic condition that currently affects nearly 2.2 million people in the United States, with more than 100,000 to 150,000 new cases reported annually. Although the onset of seizures can occur at any age, incidence rates peak in neonates and young children, plateau, then rise again in the older adult population. In the United States, the prevalence of seizures is approximately 5 to 10 cases per 1000 persons in the general population; the lifetime risk for development of epilepsy is 1 in 27 people.1 A single seizure may result from discrete, temporary abnormalities, such as a high fever in small children, hyperventilation (in susceptible patients), or alcohol withdrawal. Causes of a first seizure leading to epilepsy include genetic factors, vascular abnormalities (e.g., ischemic strokes, hemorrhages, arteriovenous malformations), significant head trauma, brain tumors, metabolic factors, and infections such as encephalitis and meningitis. Strokes are a common cause of epilepsy, particularly in the elderly. Changes in levels of various electrolytes, in particular hyponatremia and hypercalcemia, may cause isolated seizures. Also, hyperglycemia and hypoglycemia can be responsible for seizure activity, especially in patients with underlying brain injuries. A first seizure may occur in the form of status epilepticus (SE). SE is currently defined as more than 30 minutes of continuous seizure activity or two or more seizures without recovery of baseline consciousness between attacks. However, owing the risk of systemic and brain injury from prolonged seizures, efforts are being made to change the definition to 5 minutes’ duration. This definition is already accepted accepted by the American Epilepsy Society.2 Genetic predisposition is strongest in generalized forms of epilepsy in which the entire brain is electrically unstable; however, the genetic and biochemical defects are only starting to be characterized. Childhood absence (petit mal) epilepsy, juvenile myoclonic epilepsy, and generalized convulsive epilepsy are syndromes with a genetic predisposition. Mutations in γ-aminobutyric acid (GABA) receptors and sodium channels have been implicated. These types of epilepsy account for approximately one third of all cases, with seizures and abnormalities on electroencephalography (EEG) affecting the entire brain. The remaining types of epilepsy are related to localization; focal electrical abnormalities are usually the result of a structural lesion. The occurrence of prolonged or complicated febrile seizures in infancy is strongly correlated with the subsequent development of temporal lobe epilepsy.3 Although the terms epilepsy and seizure disorder are often used interchangeably, they have two distinct definitions. A seizure can be defined as an isolated event in which a group of neurons produces excessive electrical discharges in the brain. Seizures occur when the balance between excitation and inhibition of the brain’s electrical activity becomes abnormally altered in favor of excitation. Seizures can be caused by the excess production or release of an excitatory neurotransmitter, which stimulates neurons to discharge abnormally, or by a loss of inhibitory neuronal activity, which permits abnormal excitation and discharges of neurons to occur. Single or even recurrent seizures can be triggered by hypoxia or other metabolic factors, but they do not constitute epilepsy unless they recur in a habitual and unprovoked manner. A subset of acute symptomatic seizures are those that occur in the setting of an acute medical illness or metabolic crisis. These conditions include hypoglycemia; nonketotic hyperglycemia; hyponatremia; hypocalcemia; magnesium levels below 0.8 mEq/L; renal failure and uremia; hyperthyroidism; disorders of porphyrin metabolism; cerebral anoxia as a complication of cardiac or respiratory arrest, carbon monoxide poisoning, drowning, or anesthetic; withdrawal states (particularly alcohol and benzodiazepine withdrawal); and drug toxicity or intoxication. Epilepsy is characterized by recurrent seizures and is divided into syndromes on the basis of various causes, seizure types, associated neurologic symptoms, anatomic correlates, age, and family history. For diagnosis and treatment, it is valuable to be able to identify both the type of seizure and the epileptic syndrome. In 1981, a commission for the International League Against Epilepsy (ILAE) developed, revised, and adopted the international classification of epileptic seizures (Box 201-1).4 Efforts were made in 2010 to revise the classification; however, the ILEA 1981 version is still widely accepted. The motivation for revising the classification is to reflect the advances being made in basic and clinical neuroscience and incorporate those advances into clinical practice.5 The classification includes two broad categories of seizure types: focal or localization related, and generalized. Focal seizures begin within networks limited to one cerebral hemisphere and show localized abnormalities on EEG. Depending on the spread of electrical activity, the patient may have varying levels of consciousness. By definition, focal seizures without impairment of consciousness, formerly known as simple partial seizures, are the aura, or warning, that the patient experiences before a larger seizure. Focal sensory seizures may be purely subjective, and focal motor seizures may involve no impairment of consciousness. If the seizure activity spreads and involves the brainstem or both hemispheres, consciousness becomes altered and the seizure is classified as complex partial, or more recently referred to as a focal seizure with impairment of consciousness. Altered consciousness and aberrations of behavior, such as automatisms (automatic repetitive movements), are usually associated with this type of seizure. If such seizures spread bilaterally and involve the motor cortex, the patient may have a secondarily generalized tonic-clonic seizure, now called a bilateral convulsive seizure.5,6 In contrast, primary generalized seizures occur when the initial abnormal electrical activity begins in both cerebral hemispheres and involves bilaterally distributed neuronal networks. These seizures are usually seen with idiopathic or hereditary types of epilepsy. Consciousness is almost always impaired, and the seizure may be convulsive or nonconvulsive. Motor activity and electroencephalographic changes are bilateral. Nonconvulsive generalized seizures, such as absence (petit mal) seizures, may be brief, and the patient may initially be diagnosed as a “daydreamer.” The electroencephalographic characteristics of generalized spike and wave patterns are crucial for the proper diagnosis of these types of seizures. Convulsive primary generalized seizures, such as tonic-clonic (grand mal) types, are rarely missed but can be confused with secondarily generalized tonic-clonic seizures. Being able to differentiate between these two types is helpful in prescribing the appropriate treatment because each type may respond differently to certain antiepileptic medications. In the case of secondarily generalized seizures, it is important to exclude an underlying structural lesion, such as a brain tumor. For treatment to be tailored to the individual, it is essential that consideration be given to the seizure type as well as the epileptic syndrome to which it belongs. The International Classification of Epilepsy and Epileptic Syndromes (Box 201-2) was adopted by the ILAE in 1989 and allows the practitioner to categorize cases by seizure type, cause, precipitating factors, age at onset, and prognosis.5 This has been further adapted to classify the cause of seizures as genetic, structural, metabolic, or unknown. Epileptic syndromes can be further classified by age of onset, cognitive and developmental antecedents, electroencephalographic features, triggers, and patterns of occurrence related to sleep.6 Although epilepsy can develop at any age, certain syndromes are more age-related than others. A variety of epileptic syndromes develop in early childhood. More than 50% and perhaps as many as 70% of childhood epilepsies, particularly the benign partial epilepsies, remit at the time of puberty.7 Idiopathic, generalized epilepsy usually manifests by 18 years of age. After the age of 18 years, focal brain processes should be suspected. Brain tumors are a prominent cause of seizures in adults, whereas strokes are often the cause of seizures that begin late in life.8 Symptomatic focal epilepsy syndromes account for 30% to 35% of all cases of epilepsy.1 Seizure manifestations can be helpful in identifying which lobe of the brain is involved. Table 201-1 outlines the general characteristics of partial seizures in relation to the region of seizure origin; however, not all seizures fit neatly into a particular syndrome. Surgical treatment is often possible if the epileptic focus is in a surgically accessible region of the brain. An accurate and detailed history is important. It is essential to obtain history not only from the patient but also from parents, relatives, or friends who have witnessed the seizures. Complicated pregnancy or childbirth, delayed childhood development, childhood diseases such as meningitis and encephalitis, significant head trauma with loss of consciousness, and family history of epilepsy are among the significant risk factors for the development of epilepsy. New-onset seizures require the determination of any recent history of headache, illness, trauma, or focal neurologic deficit. An accurate description is important in attempting to decide whether an event was a seizure. The patient should be questioned to determine whether there was a warning before the event. A gastric sensation or a feeling of déjà vu is characteristic of temporal lobe epilepsy. A history of incontinence, injury, tongue biting, postictal confusion, lateralized weakness, or severe headache should raise suspicion of a true epileptic event. A detailed seizure history can also suggest where the seizures are originating, define seizure characteristics and frequency, and determine how the seizures are interfering with the patient’s life. A first seizure may appear in the form of SE. Immediate emergency department referral or physician consultation is indicated for SE or new-onset seizures. A general physical examination should be performed on all patients with epilepsy and should be directed toward specific disease processes and focal neurologic deficits. Skin and mucous membranes should be assessed to identify areas of injury that may be related to events that occurred while consciousness was altered. Tongue biting and cheek biting are common during tonic-clonic seizures; the tongue and cheek are usually bitten on just one side, but bilateral findings are not uncommon. If the tip of the tongue is bitten, it should give rise to the suspicion of a non-epileptic psychogenic seizure. Cardiovascular assessment is important because syncope and arrhythmias are included in the differential diagnosis of epilepsy. Postural vital signs will determine whether orthostatic hypotension is a consideration. Neurologic signs, such as lateralized weakness, papilledema, memory problems, or changes in reflexes, can signify a structural lesion in the brain. In general, a patient with epilepsy will have unremarkable physical examination findings. Clinical presentation, physical examination, and differential considerations guide diagnostic testing. A new seizure may signify a serious pathologic condition. If infection of the CNS is suspected (see Chapter 197), a complete blood count (CBC) and differential and a lumbar puncture are indicated. A chemistry profile, including calcium magnesium and phosphate, is necessary to exclude hypoglycemia, electrolyte abnormalities, or renal failure. Liver function tests (LFTs) should be performed to exclude hepatic failure. Alcohol and drug levels may be indicated. Magnetic resonance imaging (MRI) or computed tomography (CT) scan is indicated if structural abnormality, tumor, trauma, or cerebrovascular accident is suspected. Electrocardiography (ECG) should be performed to ascertain the presence of arrhythmias or heart block. Diagnosis and classification of epilepsy and seizure types require confirmation that the patient does indeed have epileptic seizures. To treat the disorder appropriately, the practitioner must attempt to determine the cause of the epilepsy and classify it according to syndrome. Appropriate diagnostic tests should be part of the initial evaluation.9 Sleep-deprived EEG is useful because a baseline recording of background brain waves may reveal epileptic abnormalities. The positive predictive value of EEG in most clinics is more than 80%, although sensitivity is only 30%.10 Because the chance of a patient having a seizure during routine EEG is small, ictal information may not be obtained; however, interictal epileptiform abnormalities may give localizing information and suggest epilepsy. Many patients with focal epilepsy show no focal or generalized abnormalities on routine EEG. Therefore a normal recording does not exclude a diagnosis of epilepsy. In contrast to focal epilepsy, generalized types of epilepsy often produce abnormalities of spike and wave activity or generalized slowing on routine electroencephalographic recordings. Interictal electroencephalographic abnormalities—either focal or generalized—are not synonymous with seizure activity, and therefore electroencephalographic abnormalities should not be the only basis for treatment. Although neuroimaging studies can be of great value in diagnosis, the absence of structural abnormalities does not exclude a diagnosis of epilepsy. CT scans are useful for identification of large mass lesions, bleeding, subdural fluid collections, and cerebral infarcts, but they often miss more subtle changes in brain structure. MRI provides extensive anatomic detail and is useful in distinguishing small low-grade tumors, scars, and neural migration disorders from one another and from normal variants in brain structure. Except in an emergency, when the immediate availability of a CT scan is an advantage, MRIs should be the primary imaging study in patients with epilepsy.9 In the preoperative evaluation of patients who are candidates for surgery, single-photon emission computerized tomography (SPECT), positron emission tomography (PET), magnetic resonance spectroscopy (MRS), functional magnetic resonance imaging (fMRI), and magnetoencephalography (MEG) are other imaging methods that may be considered.9
Seizure Disorder
Definition and Epidemiology
 Physician consultation is indicated for suspected central nervous system (CNS) lesions, SE, initiation of antiepileptic medications, treatment failures, and women with epilepsy who are contemplating pregnancy.
Physician consultation is indicated for suspected central nervous system (CNS) lesions, SE, initiation of antiepileptic medications, treatment failures, and women with epilepsy who are contemplating pregnancy.
Pathophysiology
Classification of Seizures, Epilepsy, and Epileptic Syndromes
Clinical Presentation
Physical Examination
Diagnostics
Seizure Disorder
Chapter 201