Chapter 110
Rapid Response Systems
Rapid Response Teams and Medical Emergency Teams
Terms and Definitions
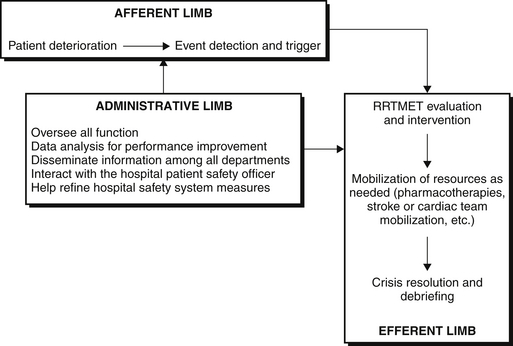
One of the goals of the first consensus conference on medical emergency teams was to unify terms used to describe these teams. A rapid response team (RRT) does not include a prescribing individual, such as a physician or advanced practitioner. These teams often are led by a nurse and may include a respiratory therapist. An RRT quickly evaluates a patient, initiates basic interventions based on standing orders or protocols, and contacts a physician or advanced practitioner, but cannot initiate advanced therapies. Medical emergency teams (METs) have the capability to prescribe new therapies and are frequently led by a physician from the intensive care unit (ICU) or emergency department. Other team members may include ICU-trained nurses, respiratory therapists, and pharmacists. Rapid response system (RRS) describes the overall infrastructure through which RRTs and METs function (Figure 110.1). The RRS includes an afferent arm, which detects signs of impending physiologic deterioration; an efferent arm (RRT or MET) and any needed resources to render treatment; and an administrative arm, which oversees the system and detects trends or recurrent events. The administrative arm collects and analyzes data related to causes of patient deterioration, optimizes methods for the early detection of patient deterioration, and ensures that adequate resources are immediately available to intervene as needed.
Building the Team
No optimal criteria for activation of MET/RRT exist. Although many scoring systems have been validated to predict in-hospital mortality or outcomes in the ICU, such as the Acute Physiology and Chronic Health Evaluation (APACHE) and the Simplified Acute Physiology Score (SAPS), none have been validated as triage tools for the bedside assessment of ward patients. The Modified Early Warning Score (MEWS) (Table 110.1) has been validated as a tool to predict the need for ICU admission and mortality in hospitalized patients. Scores of 4 or more are associated with increased mortality and admission to the ICU with a demonstrated sensitivity of 75% and specificity of 83%. Although criteria for activation of the MET/RRT are most often based on physiologic signs, it is imperative to emphasize the importance of medical staff discretion in activating the team (Box 110.1). Since 2009, the JC has stipulated that patients and families also have a means to quickly solicit help from hospital health care providers if the patient or a family member perceives a significant, acute change in the patient’s medical condition.














