![]() Emergent venous access for fluid resuscitation or drug infusion if alternative peripheral or central access is either unattainable or contraindicated
Emergent venous access for fluid resuscitation or drug infusion if alternative peripheral or central access is either unattainable or contraindicated
CONTRAINDICATIONS
![]() Absolute Contraindications
Absolute Contraindications
![]() Major blunt, long-bone fracture or penetrating trauma proximal to site of cutdown
Major blunt, long-bone fracture or penetrating trauma proximal to site of cutdown
![]() Relative Contraindications
Relative Contraindications
![]() Suspected proximal vascular injury (in the extremity or inferior vena cava)
Suspected proximal vascular injury (in the extremity or inferior vena cava)
![]() Overlying infection, burn, or skin damage at the site of cutdown
Overlying infection, burn, or skin damage at the site of cutdown
![]() Coagulopathy
Coagulopathy
RISKS/CONSENT ISSUES
![]() Pain (local anesthesia can be given)
Pain (local anesthesia can be given)
![]() Local bleeding and hematoma
Local bleeding and hematoma
![]() Infection (sterile technique will be utilized)
Infection (sterile technique will be utilized)
![]() General Basic Steps
General Basic Steps
![]() Analgesia
Analgesia
![]() Isolate
Isolate
![]() Stabilize
Stabilize
![]() Cannulate
Cannulate
![]() Secure
Secure
LANDMARKS
Greater saphenous vein is most easily accessible 1 to 2 cm anterior and 1 to 2 cm superior to the medial malleolus. The vein may be palpable in a nonhypotensive patient (FIGURE 26.1).
SUPPLIES
![]() Povidone–iodine or chlorhexidine solution
Povidone–iodine or chlorhexidine solution
![]() Anesthetic supplies: 1% lidocaine, 1 vial, 10-mL syringe, 22- or 25-gauge needle
Anesthetic supplies: 1% lidocaine, 1 vial, 10-mL syringe, 22- or 25-gauge needle
![]() No. 10 and no. 11 scalpel blades
No. 10 and no. 11 scalpel blades
![]() Curved Kelley hemostat
Curved Kelley hemostat
![]() Catheter-over-the-needle, 16 or 18 gauge
Catheter-over-the-needle, 16 or 18 gauge
![]() Needle driver
Needle driver
![]() Silk sutures (3-0 and 4-0), nylon suture (4-0)
Silk sutures (3-0 and 4-0), nylon suture (4-0)
![]() Iris scissors
Iris scissors
![]() Intravenous tubing and injectable sterile saline
Intravenous tubing and injectable sterile saline
![]() Wound dressing supplies
Wound dressing supplies
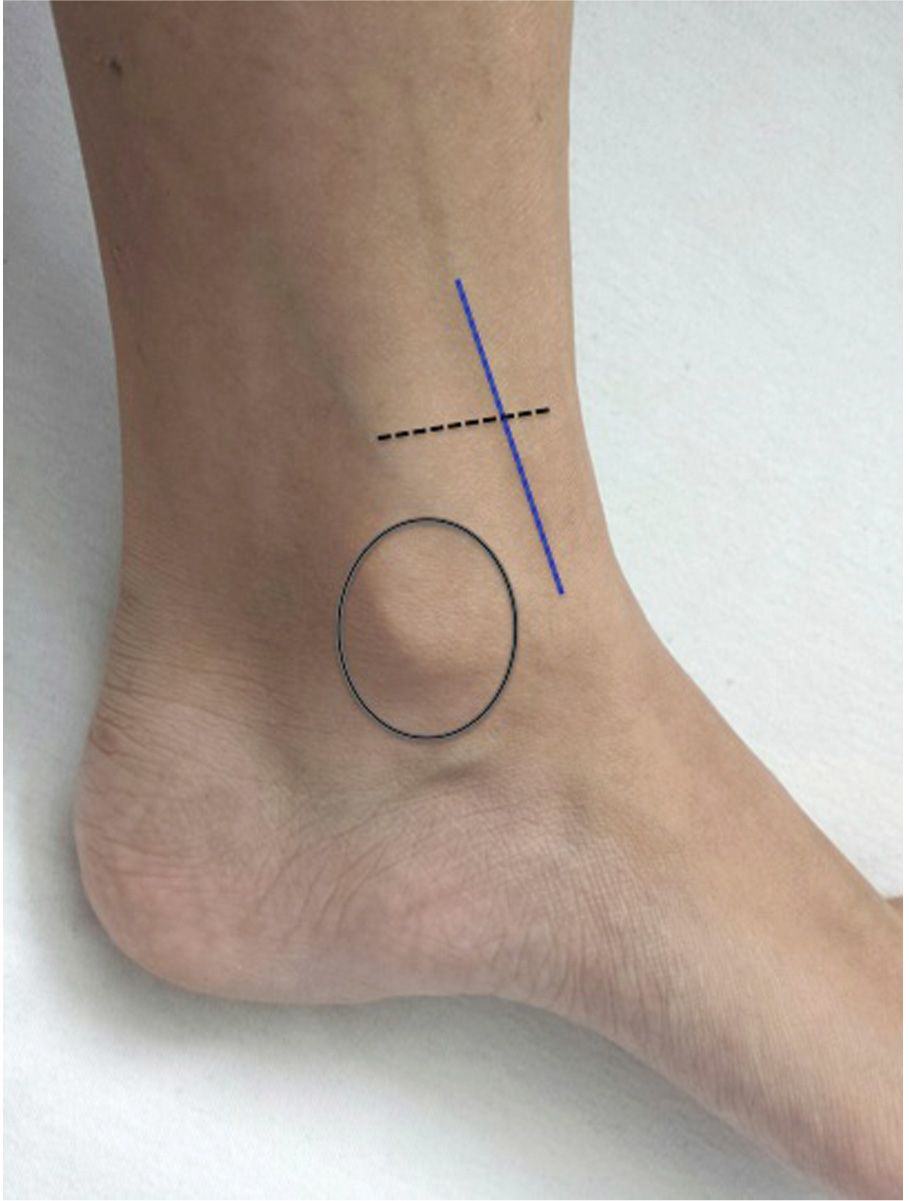
FIGURE 26.1 Saphenous vein runs vertically 2 cm anterior to the medial malleolus of the ankle. The ideal site of cutdown is 2 cm superior to the medial malleolus (dotted lines).
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Extend and externally rotate lower extremity
Extend and externally rotate lower extremity
![]() Immobilize if needed, especially in children
Immobilize if needed, especially in children
![]() Sterilize entire ankle with povidone–iodine solution and drape
Sterilize entire ankle with povidone–iodine solution and drape
Note: Unless immediate emergent access is warranted, universal precautions (cap, eye shields, mask, sterile gown and gloves) should be worn.
![]() Analgesia
Analgesia
![]() Use 25- or 27-gauge needle to anesthetize skin and subcutaneous tissue with 1% lidocaine
Use 25- or 27-gauge needle to anesthetize skin and subcutaneous tissue with 1% lidocaine
![]() Isolate: FIGURES 26.2A and B
Isolate: FIGURES 26.2A and B
![]() Make a skin incision transversely over saphenous vein landmark
Make a skin incision transversely over saphenous vein landmark
![]() Apply traction to skin on either side of the incision to expose subcutaneous tissue
Apply traction to skin on either side of the incision to expose subcutaneous tissue
![]() Dissect the subcutaneous tissue using a curved hemostat with the tip facing downward, parallel to the course of the vein
Dissect the subcutaneous tissue using a curved hemostat with the tip facing downward, parallel to the course of the vein
![]() After exposing the vein, pass the hemostat under the vein, turn the tip upward, and spread to isolate the vein above the hemostat
After exposing the vein, pass the hemostat under the vein, turn the tip upward, and spread to isolate the vein above the hemostat
![]() Stabilize: FIGURE 26.2C
Stabilize: FIGURE 26.2C
![]() Pass two 3-0 or 4-0 silk suture ties under the vein using the curved hemostat
Pass two 3-0 or 4-0 silk suture ties under the vein using the curved hemostat
![]() Clamp each tie with hemostats, one proximally and the other distally
Clamp each tie with hemostats, one proximally and the other distally
![]() Distal suture may be tied to ligate the vessel. This decreases bleeding, but also sacrifices the vessel.
Distal suture may be tied to ligate the vessel. This decreases bleeding, but also sacrifices the vessel.
![]() Apply traction on each tie, thereby lifting the vessel and exposing the anterior surface of the vein
Apply traction on each tie, thereby lifting the vessel and exposing the anterior surface of the vein
![]() Cannulate: FIGURES 26.2D and E
Cannulate: FIGURES 26.2D and E
![]() With the tip of no. 11 scalpel blade make a flap incision to the anterior surface of the vein, approximately one-third the diameter of the vein
With the tip of no. 11 scalpel blade make a flap incision to the anterior surface of the vein, approximately one-third the diameter of the vein
![]() A vein pick may be used to elevate the flap
A vein pick may be used to elevate the flap
![]() Carefully advance the catheter through the incision
Carefully advance the catheter through the incision
![]() Flush the catheter with saline solution and attach to intravenous line
Flush the catheter with saline solution and attach to intravenous line
![]() Secure Catheter: FIGURE 26.2F
Secure Catheter: FIGURE 26.2F
![]() Tie the proximal suture around the vein and the IV catheter to secure in place
Tie the proximal suture around the vein and the IV catheter to secure in place
![]() Cut the ends of the proximal and distal ties
Cut the ends of the proximal and distal ties
![]() Suture the catheter to the skin and close the incision using 4-0 nylon sutures
Suture the catheter to the skin and close the incision using 4-0 nylon sutures
![]() Cover skin insertion site with antibiotic ointment and sterile dressing
Cover skin insertion site with antibiotic ointment and sterile dressing
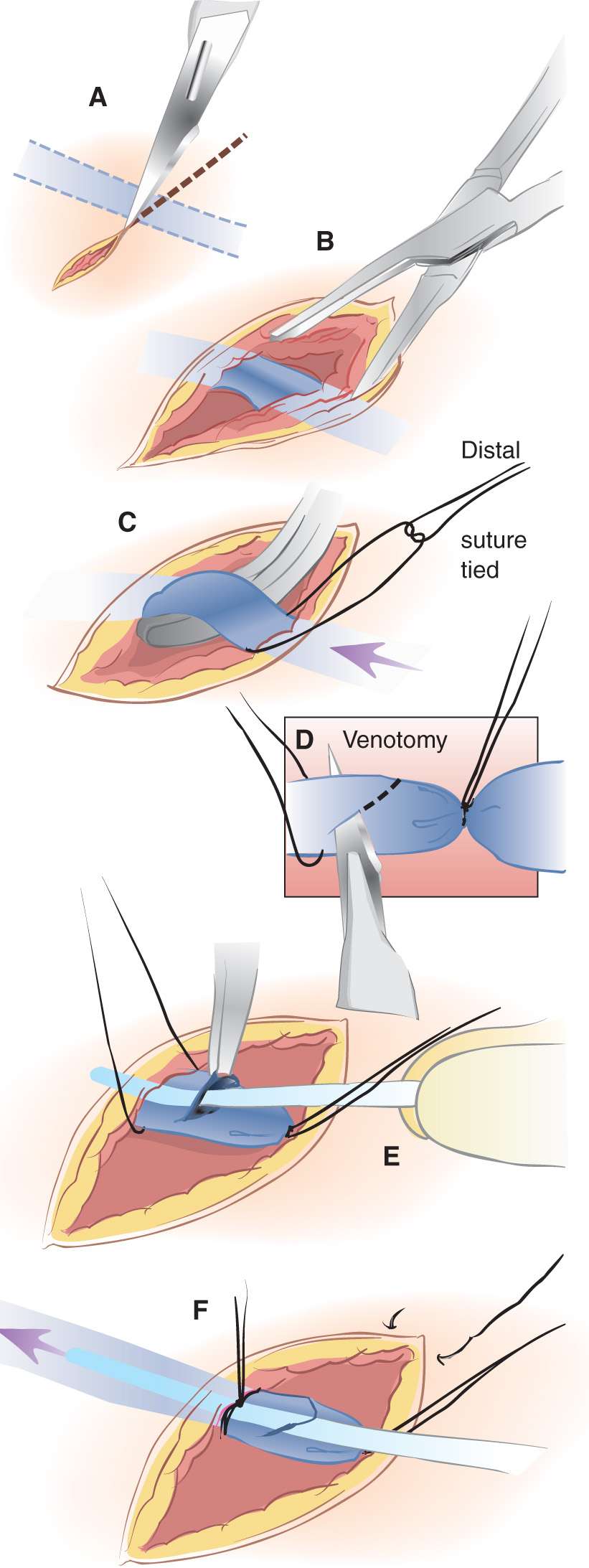
FIGURE 26.2 Procedures for venous cutdown catheterization. A: A transverse incision is made 2 cm anterior and superior to medial malleolus. The incision should extend into the subcutaneous tissue but not deep enough to potentially lacerate the vein. B: The vein is isolated using blunt dissection. A suture is passed around the vein and cut to give two ligatures. C: The distal suture is tied and used to stabilize the vessel. D: Venotomy is performed to allow insertion of the catheter. Alternatively the surgeon may choose to insert the catheter over a needle without performing a venotomy, in a manner similar to percutaneous catheterization. E: The catheter is inserted into the vein. Placement within the vessel is confirmed by aspirating blood or infusing fluid. F: The proximal suture is tied and the wound is closed and dressed. (From Vinci RJ. Venous cutdown catheterization. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:284, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


