28 Gaining vascular access promptly in the pre-hospital environment is imperative for fluid resuscitation and for the administration of intravenous drugs in critically unwell patients. Traditionally, circulatory access is gained by inserting a large-bore (14G–16G) cannula in the antecubital fossa. Suitable alternatives include the long saphenous vein, veins in the medial forearm, the dorsum of the hand and the feet. Ideally, two separate points of venous access should be obtained in different limbs, avoiding injured limbs and the arm ipsilateral to any chest injuries. In the case of suspected pelvic or inferior vena cava disruption, make sure that there is good access in place above the diaphragm. Always maximise the chances of a successful first attempt by applying a venous tourniquet no more than 10 cm from the point of cannulation. Giving it time to work and having a trusted assistant hold the limb still will also help. If this fails, consider cannulating central veins: the subclavian, external jugular and femoral are options. This must be only attempted by enhanced care teams. Another option is to obtain small vein access and infuse 50–100 mL of fluid, keeping the tourniquet on, to dilate larger proximal veins which were previously inaccessible or less obvious. If obtaining access is difficult, consider whether or not the patient absolutely requires immediate venous access in the field. Some casualties may not require urgent intravenous fluids or medication and so further attempts at siting a line can be carried out en route to hospital.
Peripheral vascular access
Importance of circulatory access
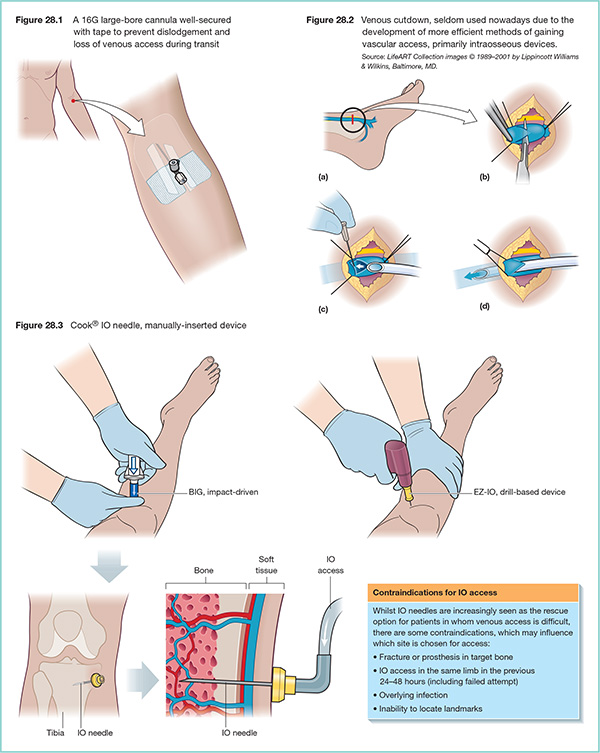
Venous access
Large-bore cannulae
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


