Ballistics
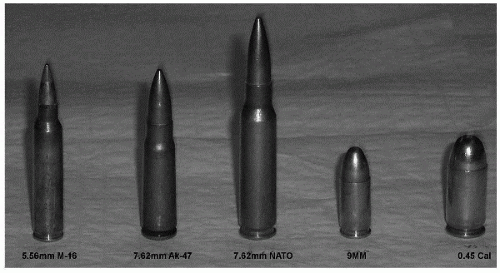
The available energy for a missile to inflict upon the body is dependent on the equation E = 1/2MV2, where M is the mass of the bullet (larger bullets impart more energy), and V is the velocity of the bullet as it hits the tissue. Thus, in most cases, the potential damage is greatest with a high-velocity round, such as that seen with a modern assault rifles and high-velocity hunting weapons.
For missile injuries, there are two areas of projectiletissue interaction. The first is a permanent cavity, which is a localized area of necrotic tissue and clot, proportional to the size of the projectile as it passes through. The second is a temporary cavity (cavitation) caused by the displacement of tissue away from the passage of the projectile. This
results in an area of contusion and concussion some distance from the actual path of the bullet. The amount of damage done to tissue depends on the amount of energy transferred to the tissue as well as the elastic properties of the tissue itself. Elastic tissues, such as skeletal muscle, blood vessels, and skin, may be displaced significantly due to cavitation but then rebound with minimal permanent injury. Inelastic tissue, such as bone, brain or liver, handles cavitation poorly and tends to fracture resulting in significant damage. There is also a shock (sonic) wave that also passes through tissue and does not cause any appreciable clinical effect (
1,
2).
Despite the fact that the energy can be imparted to a tissue is potentially most dependent on V
2 the commonly held belief that high-velocity rounds always cause increased tissue damage is incorrect. Velocity is one factor in wounding. An increase in velocity does not de facto increase the amount of tissue damage. High-velocity rounds, if they do not impact bone or relatively inelastic tissues, such as brain or solid organs (liver), shatter or yaw in the tissue they may pass through the body, imparting little destructive energy (
3). For example, the amount of tissue damage in the first 12 cm of a M-16A1 bullet wound has relatively little soft tissue disruption, similar to that of a 0.22 caliber long rifle bullet, which has less than half the velocity (
4). Although the human thigh is approximately 12 cm wide in the average individual, it can be seen that a high-velocity round may pass through the body before it imparts any significant energy outside of the bullet path.
It has been suggested that high-velocity bullets will yaw in the tissue, increasing damage. Projectiles yaw in flight, which can create irregular wounds; however, unless a projectile hits an intermediate target, the amount of yaw in flight is insignificant. Yaw, in tissue, is in fact also seldom a consideration, as the bullets will not yaw until it penetrates deeply into the body. The AK-47 bullet, for example, yaws, but not until it has penetrated 25 cm into tissue (thus, in most cases, the bullet has already passed through the body before it has reached a depth sufficient to yaw) (
5). The AK-74 assault rifle round, however, does yaw relatively early (about 7 cm of penetration), which may cause increased tissue damage.
Fragmentation of a bullet will also lead to increased tissue damage. The bullet fragments deviate out of the original bullet path in a multitude of directions and velocities causing damage to all the tissue they pass through. Although full metal jacket military rounds, in accordance with the Hauge agreement of 1899, are designed to remain intact in the body and many will, in fact, fragment after a certain distance in tissue. For example, the M-193 bullet of the M-16A1 rifle reliably fragments after traversing about 12 cm of soft tissue (
6). Thus, again the bullet may have passed through the body before it fragments or if it enters tissue >12 cm in depth, it may cause significant damage due to multiple fragments formed. Military rounds and assault rifles are designed to wound (although often severely) rather than kill, because wounded individuals require greater resources to evacuate and care for than those killed outright (
7).
It has been often stated that exit wounds are always greater than entrance wounds. This has been shown to be frequently not the case and has no bearing on care, which is always in response to the wound regardless of whether it is an entrance or exit wound (
8).
Explosive
An explosion is caused by the rapid chemical conversion of a liquid or solid material into a gas with a resultant kinetic energy release. Low-kinetic explosives (gunpowder) release energy slowly by a process called deflagration. In contrast, high-kinetic explosive detonation involves the almost instantaneous transformation of the physical space occupied by the original solid or liquid material into gases, filling the same volume within a few microseconds, and is, therefore, under extremely high pressure (
Fig. 10.1). The highly pressurized gasses expand rapidly and compress the surrounding environment, generating a pressure pulse, which is propagated as a blast wave. This blast wave is called overpressure or blast wind. As a blast wave passes through the body, it causes damage by several different mechanisms. Patients injured from explosions usually suffer from a combination of blast, blunt, penetrating, and burn trauma (
Table 10.1).
Propagation of overpressure waves down range is dependent on the environment. There are several related phenomena of a blast waves that can cause considerably more damage to the victim. Coupling occurs when one blast wave converges with another or multiple waves. The waves are additive in their destructive nature to the tissue. Reflected waves occur when the explosive force reflects off of a structures or surfaces. Both of these types of waves usually occur together in closed spaces such as buses, buildings, or streets between buildings. The cumulative force exerted on the body from reflected and coupled wave’s increases the risk of primary blast injuries. The caregiver has to have a high clinic index of suspicion when evaluating these patients exposed to such situations.
Tympanic membrane (TM) rupture is a good marker for significant exposure to blast waves. The average kinetics necessary to incur such an injury can also cause occult or delayed primary blast injuries. When a ruptured,
TM is seen in a patient exposed to explosive forces, a thorough evaluation needs to be performed even in the absence of significant injuries. Delayed presentations of occult bowel wall, pulmonary, and neurological injuries are common. Observation and repeated assessment needs to be performed for approximately 24 hours as most occult injuries will be recognized during this time.