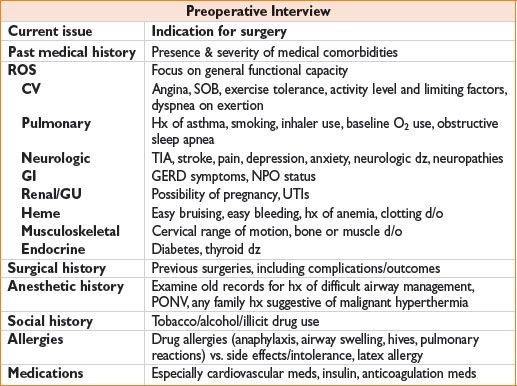
PREOPERATIVE PHYSICAL EXAMINATION
• Vital signs: Resting heart rate, BP, SpO2 height, weight, body mass index
• CV & pulm: Heart & lung sounds, JVD, pulm/periph edema, carotid bruits
• Airway examination:
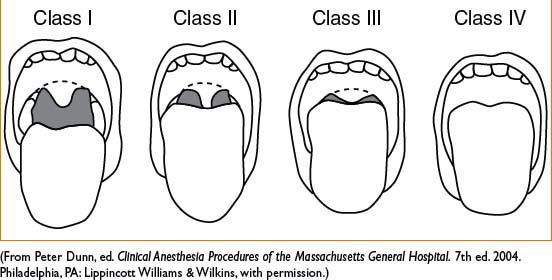
• Mallampati score (see later)
• Thyromental distance: Have pt extend neck & measure space between mental prominence and thyroid cartilage; <6 cm may indicate difficult intubation
• Cervical spine flexion/extension: Examine patient for ↓ range of motion that might limit head movement into sniffing position during intubation
• Miscellaneous: Oral opening, size of mandible (micrognathia) & tongue (macroglossia), dentition (loose, missing, prostheses)
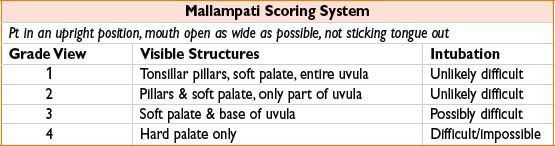
Figure 1-1. Mallampati classification of the oropharyngeal structures.
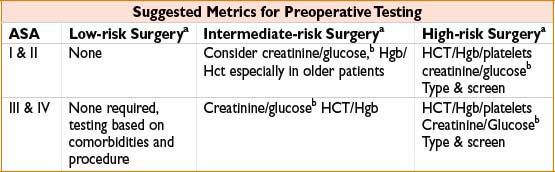
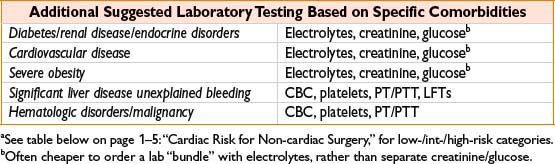
PREOPERATIVE LABORATORY TESTING
• No test is absolutely required for anesthesia, especially for healthy patients
• Consider pregnancy testing if possibility of pregnancy
• Consider creatinine if contrast will be used
• Order HCT/Hgb, type & screen if significant blood loss anticipated
ELECTROCARDIOGRAM (ECG) TESTING
• Need diagnosis other than “preoperative eval;” age-based ordering not reimbursed
• ECG indicated for:
• Symptoms or findings: Such as chest pain, syncope, palpitations, dyspnea, irregular pulse, murmur, peripheral edema, rales, suspected or recent MI/unstable angina
• Risk stratification/modification:
• Pts undergoing vascular surgery
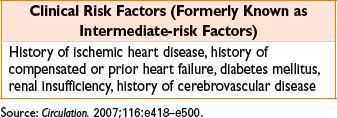
• Pts with at least 1 clinical risk factor (CAD, CVD, PVD, diabetes, Cr >2) undergoing intermediate- or high-risk surgery
• ECG NOT indicated in asymptomatic patient undergoing low-risk surgery
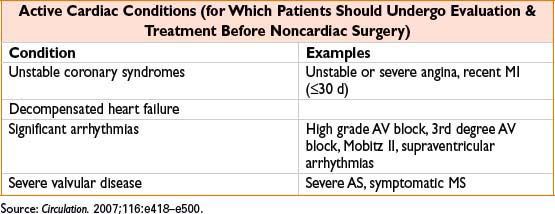
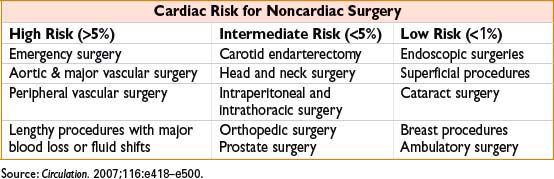
CARDIAC RISK STRATIFICATION
Figure 1-2. Perioperative risk-assessment algorithm.
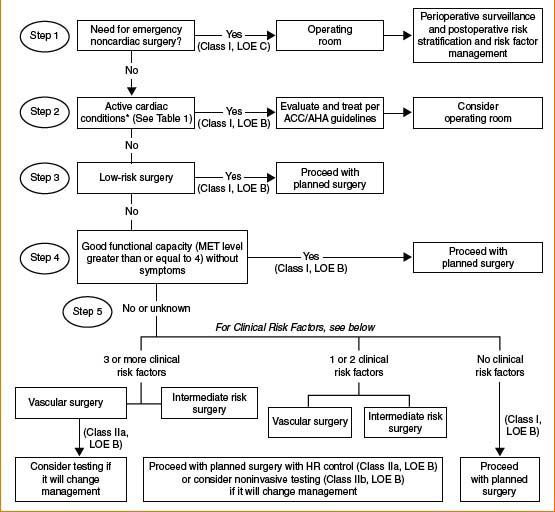
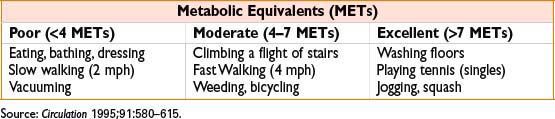
Cardiac eval algorithm for noncardiac surgery based on active clinical conditions, known cardiovascular dz, or cardiac risk factors for pts ≥50 yrs. See following tables for Active Cardiac Conditions, Clinical Risk Factors, and Metabolic Equivalents. Consider noninvasive testing before surgery in specific pts with risk factors if it will change management. HR, heart rate; LOE, level of evidence; MET, metabolic equivalent.
(Adapted from Fleisher LA, et al. ACC/AHA 2007 Perioperative Guidelines. J Am Coll Cardiol 2007;50(17):1707–1732.)
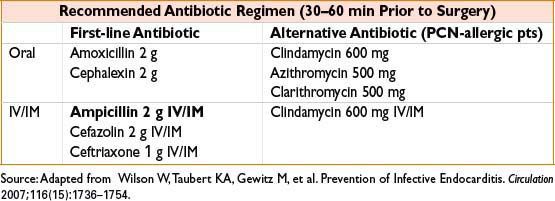
INFECTIVE ENDOCARDITIS (IE) ANTIBIOTIC PROPHYLAXIS
• Based on risk of developing IE & severity of outcome if IE were to occur
• Highest-risk patients (those requiring prophylaxis) include those with:
• Prosthetic cardiac valve or previous IE
• Congenital heart disease
• Repaired CHD with residual defect at site
• Previous cardiac transplantation with subsequent cardiac valvulopathy
Note: Guidelines no longer include pts with common valve lesions (bicuspid aortic valve, acquired aortic/mitral valve dz, mitral valve prolapse, hypertrophic cardiomyopathy)
PERIOPERATIVE β-BLOCKER THERAPY (EURO HEART J. SUPPL., 2009;11:A9–A14)
• Perioperative β-blockers may ↓ cardiac events and mortality, but may increase risk of ischemic stroke (POISE study, 2008).
• Pts already on β-blocker therapy should continue
• Time of initiation of β-blocker and specific dose still controversial
• Consider initiation of β-blocker therapy in: Intermediate- and high-risk vascular surgery patients
STATINS (2009 ACCF/AHA Perioperative Guidelines)
• Continue in the perioperative period, including day of surgery
STENTS & ANTIPLATELET AGENTS (2007 ACCF/AHA PERIOPERATIVE GUIDELINES)
• Bare metal stent: Clopidogrel & aspirin (dual antiplatelet) therapy should be continued for ≥4 wks
• Drug-eluting stent: Need ≥12 mos of dual antiplatelet therapy
• Aspirin (≥81 mg qd) should be continued perioperatively if clopidogrel is discontinued ( J. Am. Coll. Card: Cardiovasc Interven. 3(2):131–142).
CONDITIONS WHICH MAY REQUIRE DELAY OF SURGERY FOR OPTIMIZATION
• Recent MI, unstable cardiac rhythm, uncontrolled or malignant hypertension
• Coagulopathy
• Hypoxia or respiratory insufficiency
• Untreated hyperthyroidism
MEDICATIONS REQUIRING SPECIAL CONSIDERATIONS IN THE PERIOPERATIVE PERIOD
• Anticoagulants: Aspirin, plavix, coumadin, argatroban—especially if coronary stents are present or regional is being considered (see Stents and Antiplatelet Agents above). Prasugrel is a platelet inhibitor which should be stopped 7 days prior to surgery.
• Diabetic medications: Insulin, metformin (see Diabetes, 24-6)
• Antihypertensives: Ace inhibitors, angiotensin receptor blockers, β-blockers
< div class='tao-gold-member'>









