![]() Paraphimosis (foreskin trapped proximal to coronal sulcus) is a urologic emergency, and reduction is always indicated when the condition is present
Paraphimosis (foreskin trapped proximal to coronal sulcus) is a urologic emergency, and reduction is always indicated when the condition is present
CONTRAINDICATIONS
![]() None
None
RISKS/CONSENT ISSUES
![]() Pain (local anesthesia will be given)
Pain (local anesthesia will be given)
![]() Local bleeding
Local bleeding
![]() Infection (sterile technique will be used)
Infection (sterile technique will be used)
![]() Scarring at site of incision/dilation (though definitive treatment will likely include circumcision, removing the scarred tissue)
Scarring at site of incision/dilation (though definitive treatment will likely include circumcision, removing the scarred tissue)
![]() Damage to glans penis and urethral meatus
Damage to glans penis and urethral meatus
![]() General Basic Steps
General Basic Steps
If manual reduction fails to restore normal anatomy, proceed to assisted manual reduction; if that fails as well, proceed to phimotic ring incision. A urologist should be contacted if manual reduction fails, and will need to be actively involved if emergency circumcision is required because of reduction failure.
![]() Patient preparation
Patient preparation
![]() Anesthesia
Anesthesia
![]() Manual reduction
Manual reduction
![]() Assisted manual reduction (FIGURE 37.1)
Assisted manual reduction (FIGURE 37.1)
![]() Phimotic ring incision
Phimotic ring incision
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Position: Supine with legs slightly abducted
Position: Supine with legs slightly abducted
![]() Consider light procedural sedation as well
Consider light procedural sedation as well
![]() Anesthesia
Anesthesia
![]() A topical anesthetic may be all that is necessary
A topical anesthetic may be all that is necessary
![]() Apply viscous lidocaine or eutectic mixture of local anesthetics (EMLA) to the inner layer of the foreskin
Apply viscous lidocaine or eutectic mixture of local anesthetics (EMLA) to the inner layer of the foreskin
![]() Also serves as a lubricant
Also serves as a lubricant
![]() If further anesthesia is necessary, progress from local, to dorsal nerve block, and, finally, to penile ring block
If further anesthesia is necessary, progress from local, to dorsal nerve block, and, finally, to penile ring block
![]() See chapter 36 for details and pictures of penile anesthesia
See chapter 36 for details and pictures of penile anesthesia
![]() When providing local anesthesia with lidocaine (without epinephrine), be sure to infiltrate into the constricting ring as well
When providing local anesthesia with lidocaine (without epinephrine), be sure to infiltrate into the constricting ring as well
![]() Manual Reduction
Manual Reduction
![]() Using your hands or an elastic bandage, manually compress the glans and foreskin for 3 to 5 minutes to remove as much edema as possible
Using your hands or an elastic bandage, manually compress the glans and foreskin for 3 to 5 minutes to remove as much edema as possible
![]() Place both thumbs on the glans penis and apply slow, steady pressure while using your other fingers just proximal to the phimotic ring to pull the foreskin over the glans penis (FIGURE 37.2)
Place both thumbs on the glans penis and apply slow, steady pressure while using your other fingers just proximal to the phimotic ring to pull the foreskin over the glans penis (FIGURE 37.2)
![]() Successful reduction occurs when the phimotic foreskin is reduced back to normal position over the glans
Successful reduction occurs when the phimotic foreskin is reduced back to normal position over the glans
![]() If unsuccessful, proceed to assisted manual reduction methods
If unsuccessful, proceed to assisted manual reduction methods
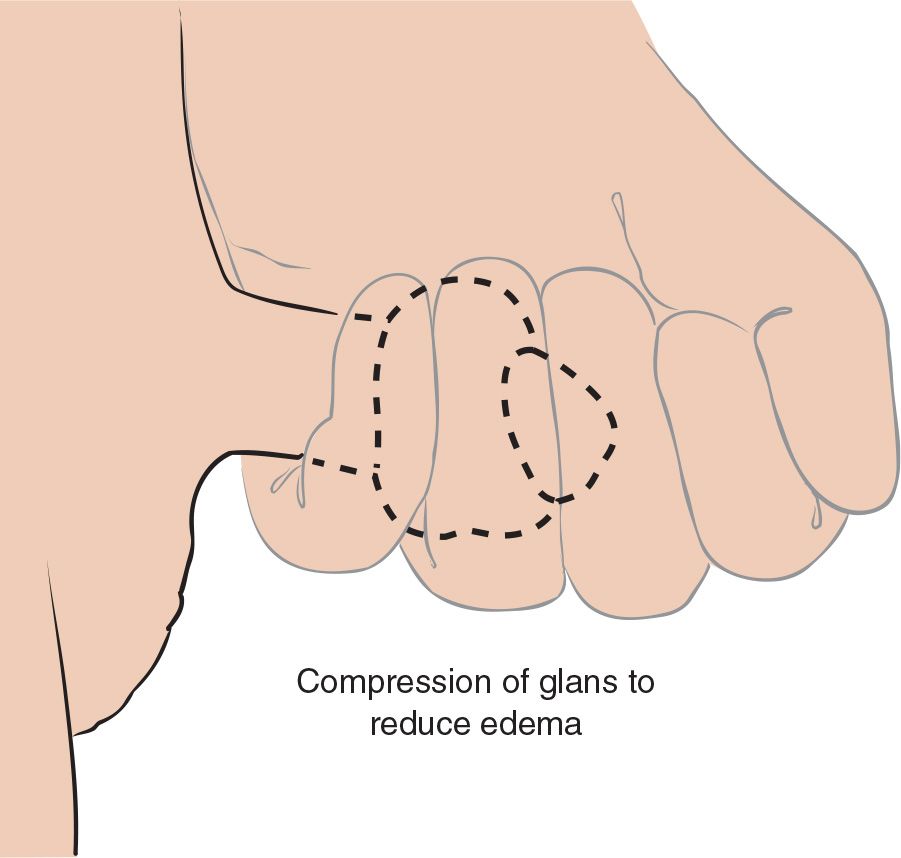
FIGURE 37.1 Technique for compression of glans to reduce edema and allow for manual reduction of paraphimosis. (From Green M, Strange GR. Paraphimosis reduction. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:1008, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


