23 The analogy that ‘children are just small adults’ is often used. However, when it comes to trauma management, there are anatomical, physiological and psychological differences that must be taken into account, although the basics remain very similar to adults. Emotional involvement can be very difficult to avoid as can bystander and parental pressure. Non-accidental injury and safeguarding issues may also be a feature. The wide range in size from a newborn to a 16 year old makes triage difficult. From a preterm infant weighing only a few kilos to an adult-sized teenager, paediatric body sizes and proportions vary vastly. Infants have a much larger head in relation to the size of their body (20%) and the relative contribution to overall body surface area decreases with age to adult proportions (10%) by adolescence. Children have a higher surface area to weight ratio than adults which means they are more susceptible to heat loss and hypothermia, in addition to fluid loss in burns. Various formulae (Figure 23.1) exist to aid estimation of weight, and equipment such as Broselow or Sandell tapes are available to assist. Children have an increased risk of airway obstruction due to large tongues, smaller mid face, smaller airway diameters, frequent respiratory tract infections and adenotonsillar hypertrophy. The larynx is higher and more anterior than adults and the narrowest point is the cricoid ring. The trachea is shorter and less rigid, making compression and endobronchial intubation more common. The large occiput in babies and young children may produce excessive flexion, causing tracheal compression and therefore neutral head positioning is used for intubation of young children. Deciduous teeth may be loose and the epiglottis is proportionately larger and more floppy. Ribs are more compliant and offer less protection to underlying organs. They are less likely to fracture than adults but there can be significant damage to underlying viscera without fracture. The smaller functional residual capacity and increased oxygen consumption make desaturation more rapid. Gastric distension can significantly compromise ventilation. Vital signs vary with age, making triage difficult (Figure 23.2). Young children have higher blood volumes per kilogram, but smaller circulating volumes overall. Assessment of neurological status is difficult in babies and young children. The AVPU system or paediatric GCS can be used. Spinal injury is less common in children due to cartilaginous vertebral bodies, elastic ligaments and more mobility of the verbal column, distributing force over a wider area Unfortunately, paediatric trauma may be the result of NAI and responders should be alert to safeguarding issues. A careful history of how the injury occurred must be taken. Any concern that the trauma may have happened as a result of NAI should be documented and relayed to the receiving hospital team. Children are more susceptible to airway obstruction and more rapid desaturation, therefore management of the airway should be performed swiftly if there is any sign of compromise. Rapid sequence intubation should only be performed by those confident in paediatric intubation within a pre-hospital setting due to the additional difficulties posed by the paediatric patient. Cuffed endotracheal tubes are safe in the short term and are more likely to be sized correctly in the first instance (Table 23.1) and they provide more airway protection where there is a risk of airway soiling or difficulties with ventilation. Care should be taken with assisted ventilation not to insufflate air into the stomach since gastric distension can splint the diaphragm and make ventilation more difficult. A nasogastric tube may be inserted after intubation to decompress the stomach. Table 23.1 Laryngeal mask airway (LMA) Signs of respiratory distress in children include use of accessory muscles, tracheal tug, grunting and nasal flaring, intercostal muscle recession, and peripheral and central cyanosis. Paediatric BVMs should be used where available with a mask of an appropriate size and with caution to avoid over-distension and barotrauma. Hypotension may not develop until 25–40% of circulating volume has been lost. Peripheral perfusion is a useful sign of circulatory compromise. Intravenous access can be difficult in young children and may be made more difficult in hypovolaemia. Intraosseous access should be considered after two attempts or more than 90 seconds of attempting intravenous access. In hypovolaemia, a 20 mg/kg fluid bolus should be given. There is no evidence of benefit from smaller fluid boluses (in the same way practitioners permit hypotension in some bleeding adults) in paediatric practice. Abdominal injuries are more likely as there is less protection for the upper abdominal organs from the compliant thoracic cage leading to an increased likelihood of splenic and liver injuries. The pelvis protects the bladder less effectively than in adults. Head injuries are common in children but assessment of neurological status may be difficult in young children. An alternative GCS scoring system adapted specifically for children may be considered for greater accuracy. Hypoglycaemia is more common in children. Assess the burn area using Lund and Browder charts which takes age into account. The rule of nines is inappropriate in young children given the larger head surface area. A child’s palm and fingers is a useful estimation of 1% total body surface area. The higher surface area to weight ratio leads to increased fluid loss from burn areas. Smaller airway diameter means that airway obstruction occurs more quickly with inhalational burns and intubation should be performed promptly. The risk of high cervical spine fractures is high due to the larger head. Weak neck muscles mean that the fulcrum of spinal flexion is C2/3 in smaller children and C5/6 in older children. Great care should be taken to immobilise children at the pre-hospital stage. Spinal cord injuries are also possible without radiological abnormalities (SCIWORA). Car seats, adult lower limb box splints and vacuum splints are useful for the immobilisation of babies and toddlers. Pain and distress should be ameliorated as quickly as possible. Use of Entonox may be considered in children old enough to be able to use it and intranasal diamorphine is a useful drug if intravenous access is difficult. Keeping parents close by is useful to reduce distress for the child and to enable consent and information gathering. Children under 16 who are deemed competent can consent to treatment (Gillick competence) but cannot refuse treatment. Emergency treatment should be provided where necessary, ideally with consent of the person with parental responsibility. However, they may not be present. Parental presence at resuscitation attempts may be beneficial and aid grieving when outcomes are unsuccessful.
Paediatric trauma
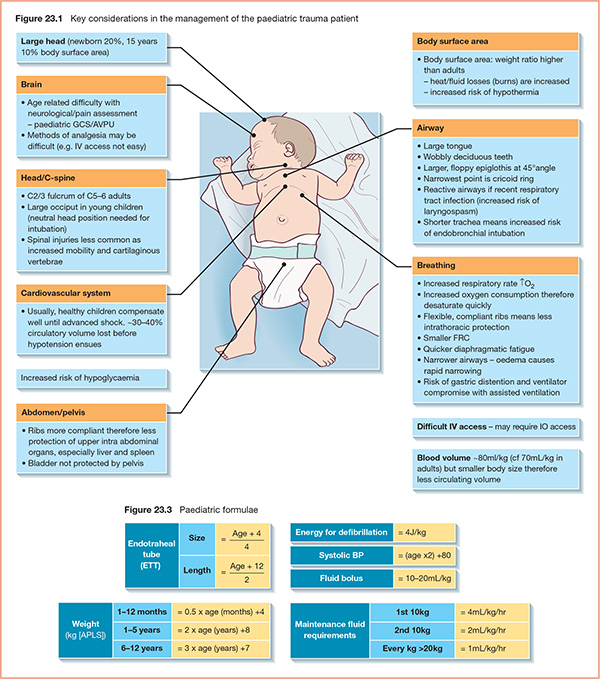
Body size and weight

Airway
Respiratory system
Cardiovascular system
Neurological system
Non-accidental injury
Paediatric primary survey
Airway
Weight (kg)
LMA size
Cuff volume (mL)
>5 kg
1
4
5–10
1.5
7
10–20
2
10
20–30
2.5
14
30–50
3
20
Breathing
Circulation
Disability
Burns
Spinal injury
Analgesia
Consent and parents
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


