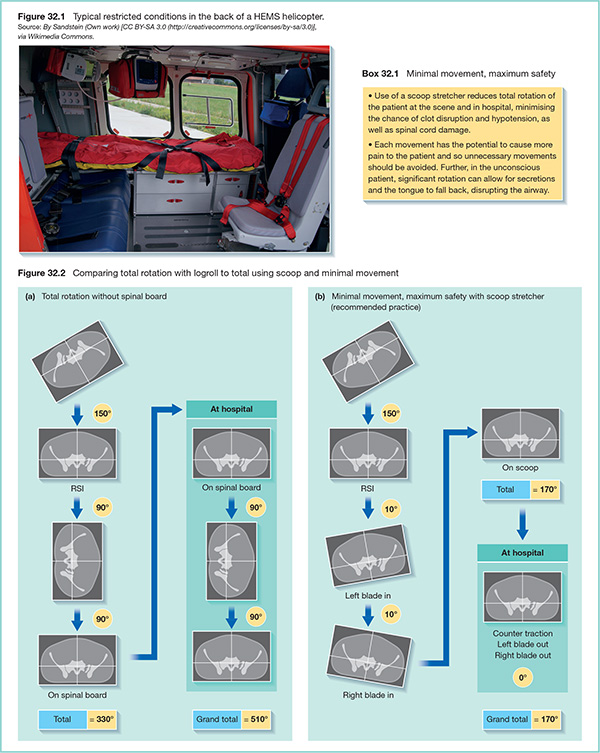
32 Innovation in pre-hospital care on-scene and in critical care at the hospital has been impressive, but the journey from the scene to the hospital remains a limiting factor. Treatment in the back of a helicopter or an ambulance can be impeded and the ability of teams to alter their management plan while in transit is highly limited. Therefore, it is crucial to ensure that the casualty is optimally prepared for transport – this is the aim of packaging. Immobilisation is key in packaging. It minimises serious pain (using bone splinting), serious morbidity (spinal cord injury) and mortality (dislodgment of formed clots). Splinting limb fractures minimises pain by eliminating unnecessary movement at fracture sites. Bringing bones back into anatomical alignment precludes the mobile ends of fractured bones from damaging blood vessels, causing further haemorrhage, and also reduces the area into which any torn blood vessels can bleed. ‘Clot and cord’ management can be grouped together, as the measures taken to prevent spinal cord damage also minimise clot disruption. Traditionally in the UK, spinal cord immobilisation involves the use of a cervical collar and blocks secured to a rigid spinal board with the patient log-rolled onto and off the board. However, in a consensus statement from the Faculty of Prehospital Care in 2013, Moss et al. (2013) have stated that the long spinal board should be used only as an extrication device, and not for patient transfer to hospital. While safeguarding against cord injury, the log-rolling required to move the patient onto and off the board risks causing further haemorrhage from disrupting the clots formed naturally (typically over a period of 10 minutes) by the patient’s coagulation cascade after trauma.
Packaging
What is packaging?
Patient-oriented packaging
Minimal movement, maximum safety
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


