65. Osteogenesis Imperfecta
Definition
Osteogenesis imperfecta (OI), one of the most common skeletal dysplasias, is inherited via autosomal dominant mutation(s). It is produced by defective biosynthesis of type I collagen, which results in brittle, osteoporotic bones that are easily fractured. Osteogenesis imperfecta is also known as Lobstein disease, brittle-bone disease, blue sclera disease, and fragile bone disease.
Incidence
Osteogenesis imperfecta is estimated to occur in 1:20,000 to 1:30,000 births.
Etiology
Type I collagen occurs naturally as a triple helix whose constituents are two copies of the α 1-chain and one copy of the α 2-chain. The pro–α 1-chain is encoded by the COL1A gene located on chromosome17, whereas the pro–α 2-chain is encoded by the COL2A gene on chromosome 2. Quantitative defects of type I collagen are the result of mutations on the COL1A gene. Qualitative defects of type I collagen result from mutations of either the COL1A or COL2B gene, producing a mixture of both normal and abnormal collagen chains. The disease does not exhibit any predilection for a particular race, ethnic group, or gender.
Signs and Symptoms
• Barrel chest
• Blue sclera
• Constipation
• Defective dentition
• Fractures
• Growth retardation
• Hearing loss
• Joint laxity
• Kyphosis
• Limb deformities
• Macrocephaly
• Scoliosis
• Sweating
• Triangular face
• Wormian bones
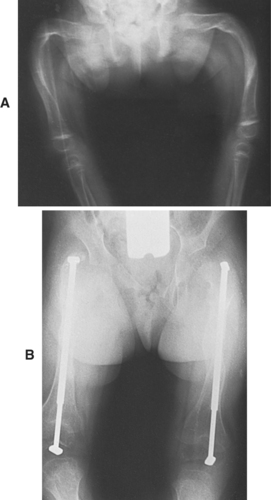 |
| Osteogenesis Imperfecta. A, Severe deformity of both femurs. B, Same individual after multiple osteotomies with telescoping medullary rod fixation. |
Medical Management
In the past, the primary interventions for OI consisted of deformity correction by surgical intervention, physiotherapy, orthotic support(s), and mobility-assistance devices, such as wheelchairs. As the molecular nature of this disease has become better understood, pharmacotherapy is being increasingly employed to augment bone mass and strength. Surgical intervention is kept in reserve for functional improvement.
Synthetic pyrophosphate analogues—such as bisphosphonates (particularly pamidronate)—inhibit osteoclast-mediated bone resorption. Because osteoblastic new bone formation is unopposed, cortical thickness increases, yielding stronger bone tissue. Intravenous administration of pamidronate is effective in infants, and its administration may ameliorate the natural course of the disease. In particular, pamidronate decreases the rate of fractures, increases bone mineral density, decreases bone pain, and contributes to increased height. Growth hormone may be given to act on the growth plate and stimulate osteoblast function. The patient with a quantitative collagen defect may derive somewhat greater benefit from growth hormone administration; however, the role of growth hormone has yet to be clearly delineated.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


