Parasagittal (oblique) view. The laminae (L) form a ‘saw-tooth’ pattern.
Parasagittal (oblique) view of L5–S1 junction.
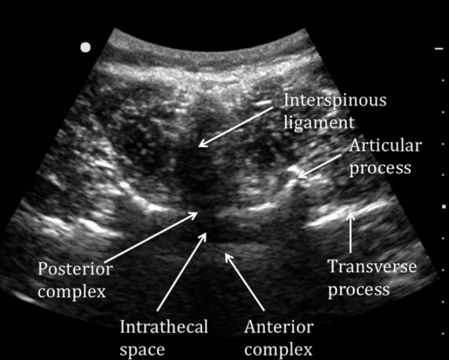
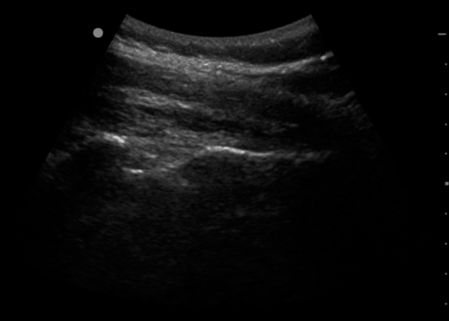
Transverse (interlaminar) view of the lumbar spine.

Transverse view showing the depth to the posterior complex.
Key points
1. Maternal obesity significantly increases both obstetric and fetal morbidity and is an independent risk factor for maternal mortality.
2. Prepregnancy BMI >40 kg/m2 and a delivery BMI >45 kg/m2 are predictive of a higher incidence of anaesthetic complications.
3. Antenatal anaesthetic assessment is recommended for parturients with BMI >40 kg/m2 at booking.
4. Early epidural placement is recommended during labour. Timing in relation to administration of LMWH may be required.
5. Spinal ultrasound may be helpful in achieving correct placement of central neuroaxial blocks.
6. Prepare for difficult laryngoscopy in the obese parturient with optimal patient positioning and an appropriate airway plan.
7. Meticulous care is required to reduce significant postoperative risks, including respiratory complications, thromboembolism and infections.
Further reading
Related posts:
 Non-regional analgesia techniques for labour
Anaesthesia for other obstetric indications: cervical suture, external cephalic version, controlled ARM, manual removal of placenta and perineal repair
Non-regional analgesia techniques for labour
Anaesthesia for other obstetric indications: cervical suture, external cephalic version, controlled ARM, manual removal of placenta and perineal repair
 Regional analgesia techniques for labour
Endocrine disease in pregnancy, including diabetes mellitus, thyroid and adrenal disease
Regional analgesia techniques for labour
Endocrine disease in pregnancy, including diabetes mellitus, thyroid and adrenal disease
 Maternal collapse, including massive obstetric haemorrhage, amniotic fluid embolism and cardiac arrest
Maternal collapse, including massive obstetric haemorrhage, amniotic fluid embolism and cardiac arrest
 Haematologic disease in pregnancy
Haematologic disease in pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


