![]() Testicular torsion
Testicular torsion
Signs and symptoms include:
![]() Acute scrotal pain/swelling or intermittent testicular pain
Acute scrotal pain/swelling or intermittent testicular pain
![]() Testicular tenderness
Testicular tenderness
![]() High-riding testis with horizontal lie
High-riding testis with horizontal lie
![]() Absent cremasteric reflex on the affected side
Absent cremasteric reflex on the affected side
![]() Negative Prehn sign (no relief of pain upon elevation of the testis)
Negative Prehn sign (no relief of pain upon elevation of the testis)
Manual detorsion may serve as a temporizing measure to reperfuse the testis while the patient is awaiting definitive surgical management. A urologist or general surgeon should be consulted immediately when torsion is suspected to prepare for emergency surgery.
CONTRAINDICATIONS
![]() Manual detorsion should not delay scrotal exploration and bilateral orchiopexy in the operating room (OR)
Manual detorsion should not delay scrotal exploration and bilateral orchiopexy in the operating room (OR)
![]() Spermatic cord anesthesia should be used only after discussing with the consulting urologist because it may blunt the subjective end point of detorsion efforts (relief of pain)
Spermatic cord anesthesia should be used only after discussing with the consulting urologist because it may blunt the subjective end point of detorsion efforts (relief of pain)
RISKS/CONSENT ISSUES
![]() Pain (sedation and local anesthesia may be used)
Pain (sedation and local anesthesia may be used)
![]() Local bleeding and/or infection if spermatic cord anesthesia is administered
Local bleeding and/or infection if spermatic cord anesthesia is administered
![]() Manual detorsion does not replace the absolute need for surgical scrotal exploration/orchiopexy
Manual detorsion does not replace the absolute need for surgical scrotal exploration/orchiopexy
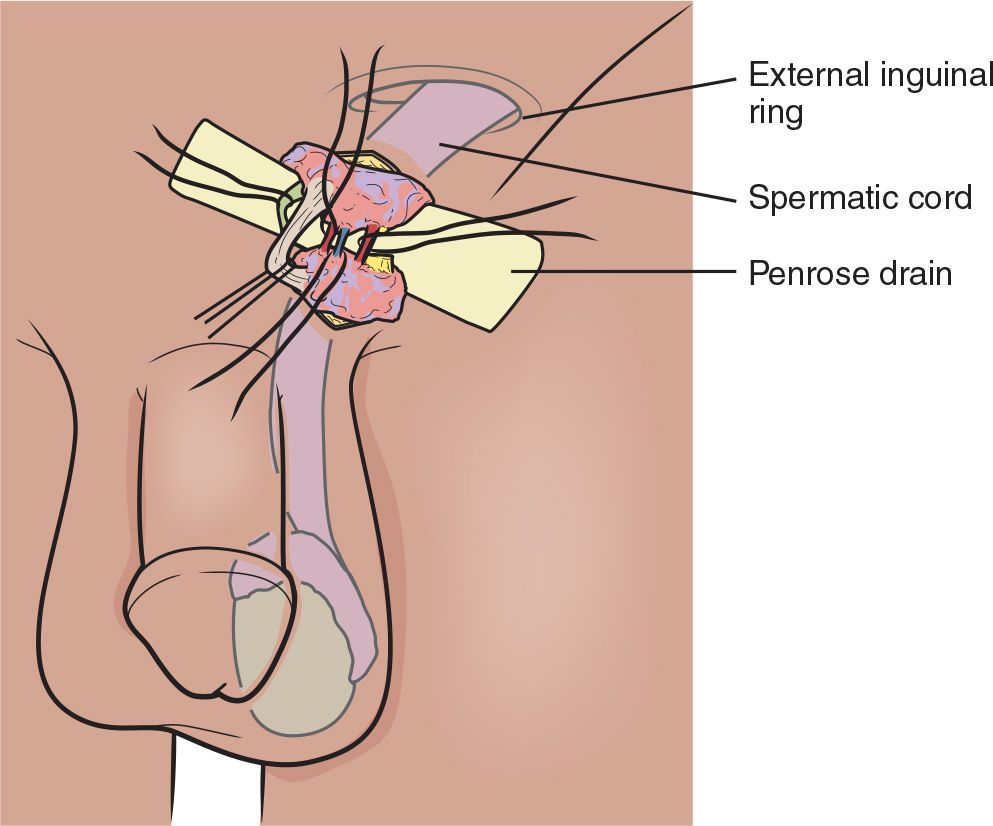
LANDMARKS
![]() If considering spermatic cord anesthesia/block, identify the spermatic cord at the external inguinal ring. Alternatively, if severe edema is present, palpate cord at pubic tubercle over pubis.
If considering spermatic cord anesthesia/block, identify the spermatic cord at the external inguinal ring. Alternatively, if severe edema is present, palpate cord at pubic tubercle over pubis.
![]() General Basic Steps
General Basic Steps
![]() Patient preparation
Patient preparation
![]() Local anesthesia (optional)
Local anesthesia (optional)
![]() Detorsion
Detorsion
![]() Confirmation
Confirmation
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Place the patient in reclining, supine, or lithotomy position
Place the patient in reclining, supine, or lithotomy position
![]() Consider light procedural sedation
Consider light procedural sedation
![]() Local Anesthesia (optional)
Local Anesthesia (optional)
![]() Ensure that the consulting urologist or general surgeon does not object to providing local anesthesia
Ensure that the consulting urologist or general surgeon does not object to providing local anesthesia
![]() Spermatic Cord Block
Spermatic Cord Block
![]() Sterilize the skin overlying the spermatic cord
Sterilize the skin overlying the spermatic cord
![]() Insert small (30-gauge) needle directly into the spermatic cord (FIGURE 35.1)
Insert small (30-gauge) needle directly into the spermatic cord (FIGURE 35.1)
![]() Aspirate for blood to ensure the needle is not intravascular
Aspirate for blood to ensure the needle is not intravascular
![]() Slowly inject 10 mL of 1% plain lidocaine (maximum 3 mg/kg)
Slowly inject 10 mL of 1% plain lidocaine (maximum 3 mg/kg)
![]() Detorsion
Detorsion
![]() The most common direction for torsion to occur is lateral to medial
The most common direction for torsion to occur is lateral to medial
![]() The initial attempt at detorsion should therefore be medial to lateral (FIGURES 35.2 and 35.3). Imagine you are “opening a book.”
The initial attempt at detorsion should therefore be medial to lateral (FIGURES 35.2 and 35.3). Imagine you are “opening a book.”
![]() Multiple rotations of the testicle may be necessary for complete detorsion; the degree of torsion may be guided by the patient’s pain relief
Multiple rotations of the testicle may be necessary for complete detorsion; the degree of torsion may be guided by the patient’s pain relief
![]() One-third of cases are torsed in the opposite direction. If initial detorsion efforts appear ineffective/painful, attempt to detorse laterally to medially.
One-third of cases are torsed in the opposite direction. If initial detorsion efforts appear ineffective/painful, attempt to detorse laterally to medially.
![]() Confirmation
Confirmation
![]() Relief of pain
Relief of pain
![]() Restoration of anatomy
Restoration of anatomy
![]() Eventual return of cremasteric reflex
Eventual return of cremasteric reflex
![]() Color Doppler ultrasonogram shows return or improvement of flow
Color Doppler ultrasonogram shows return or improvement of flow
COMPLICATIONS
![]() Unsuccessful manual detorsion
Unsuccessful manual detorsion
![]() Patient unable to tolerate procedure (consider procedural sedation)
Patient unable to tolerate procedure (consider procedural sedation)
![]() Testicular loss due to prolonged ischemia
Testicular loss due to prolonged ischemia
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


