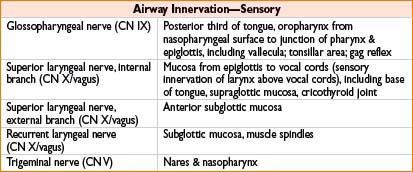
• Injury of SLN (external branch) → hoarseness
• Injury of RLN → unilateral paralysis → paralysis of ipsilateral vocal cord → hoarse voice; bilateral paralysis → stridor & respiratory distress
Airway Assessment
• History
• Adverse events related to prior airway management
• Radiation/surgical history
• Burns/swelling/tumor/masses
• Obstructive sleep apnea (snoring)
• Temporomandibular joint dysfunction
• Dysphagia
• Problems with phonation
• C-spine disease (disk dz, osteoarthritis, rheumatoid arthritis, Down’s syndrome)
• Physical examination
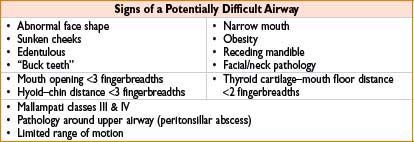
• Mallampati score (see also Chapter 1, Preoperative Assessment)
• Symmetry of mouth opening
• Loose/missing/cracked/implanted teeth
• Macroglossia (associated with difficult laryngoscopy)
• High-arched palate (associated with difficulty visualizing larynx)
• Mandible size
• Thyromental distance <3 fingerbreadths suggests poor laryngeal visualization
• Neck examination
• Prior surgeries/tracheostomy scars
• Abnormal masses (hematoma, abscess, goiter, tumor) or tracheal deviation
• Neck circumference & length
• Range of motion (flexion/extension/rotation)

Airway Devices
• Oral and nasal airways
• Typically inserted secondary to loss of upper airway muscle tone in anesthetized patients → usually caused by tongue or epiglottis falling against posterior pharyngeal wall
• Length of nasal airway estimated by measuring from nares to meatus of ear
• Use caution with insertion in pts on anticoagulation or with basilar skull fractures
• Mask airway
• Facilitates O2 delivery (denitrogenation) as well as anesthetic gas using airtight seal
• Hold mask with left hand while right hand generates positive-pressure ventilation → (use <20 cm H2O to avoid gastric inflation)
• One-handed technique
• Fit snugly around bridge of nose to below bottom lip
• Downward pressure with left thumb & index finger, middle, & ring finger; grasp the mandible while pinky finger is placed under angle of jaw to thrust anteriorly
• Two-handed technique
• Used in difficult ventilatory situations
• Bilateral thumbs hold mask down while fingertips displace jaw anteriorly
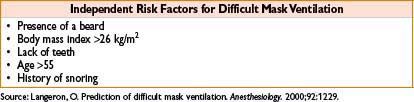
• Edentulous patients may be a challenge to ventilate (difficult to create a mask seal) → consider leaving dentures in place, oral airway, buccal cavity gauze packing
• Difficult mask ventilation: Maneuvers to maintain airway patency
• Call for additional help (have someone else squeeze bag)
• Insert oral and or nasal airways
• Extend neck & rotate head
• Perform jaw thrust
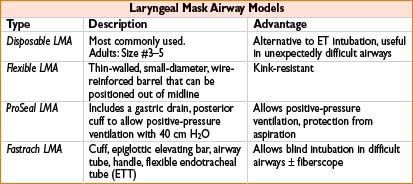
• Supraglottic airways (laryngeal mask airways)
• Insertion technique:
• Patient placed in sniffing position
• Deflated LMA cuff is lubricated & inserted blindly to hypopharynx
• Cuff is inflated to create a seal around entrance to larynx
• (Tip rests over upper esophageal sphincter, cuff upper border against base of tongue, sides lying over pyriform fossae)
• Indications
• Alternative to endotracheal intubation (not as a replacement) or mask ventilation
• Rescue device in expected/unexpected difficult airway
• Conduit for intubating stylet, flexible FOB, or small diameter ET
• Contraindications: Pharyngeal pathology, obstruction, high aspiration risk, low pulmonary compliance (need peak inspiratory pressures >20 cm H2O), long surgeries
• Disadvantages: Do not protect the airway, can become dislodged
• Endotracheal tubes (ETTs)
• Used to deliver anesthetic gas directly to trachea & provide controlled ventilation
• Modified for a variety of specialized applications: Flexible, spiral-wound, wire-reinforced (armored), rubber, microlaryngeal, oral/nasal RAE (preformed), double-lumen tubes
• Airflow resistance depends on tube diameter, curvature, length
• All ETTs have an imprinted line that is opaque on radiographs

• Rigid laryngoscopes: Used to examine larynx & facilitate tracheal intubation
• Macintosh blade (curved): Tip inserted into vallecula; use size 3 blade for most adults
• Miller blade (straight): Tip inserted beneath laryngeal surface of epiglottis; use size 2 blade for most adults
• Modified laryngoscopes: Wu, Bullard, & Glidescope for use in difficult airways
• Flexible fiberoptic bronchoscopes
• Indications: Potentially difficult laryngoscopy/mask ventilation, unstable cervical spines, poor cervical range of motion, TMJ dysfunction, congenital/acquired upper airway anomalies
• Light wand
• Malleable stylet with light emanating from distal tip, over which ETT is inserted
• Dim lights in OR & advanced wand blindly
• Glow in lateral neck → tip in piriform fossa
• Glow in the anterior neck → correctly positioned in trachea
• Glow diminishes significantly → tip likely in esophagus
• Retrograde tracheal intubation
• Performed in awake & spontaneously ventilating pts
• Puncture cricothyroid membrane with 18-gauge needle
• Introduce guidewire & advanced cephalad (use 80 cm, 0.025 in. wire)
• Visualize wire with direct laryngoscopy & guide ETT through vocal cords
• Airway bougie
• Solid or hollow, semimalleable stylets usually passed blindly into trachea
• ETT is threaded over bougie into trachea; can feel “clicking” as passes over tracheal rings
• May have internal lumen to allow for insufflation of O2 & detection of CO2
• Video laryngoscopes (Glidescope®, Storz® V-Mac™, and McGrath®)
• Usually a MAC style blade with a camera at the distal tip attached to a mobile video screen
• Assists with anterior airways, useful in obese pt; usually improves the view of the glottic opening; however, sometimes difficult to pass the ETT, unless a curved stylette is utilized

AIRWAY MANAGEMENT: OROTRACHEAL INTUBATION
• Elevate height of bed to laryngoscopist’s xiphoid process
• Place patient in sniffing position: Neck flexion, head extension; aligns oral, pharyngeal, & laryngeal axes to provide the straightest view from lips to glottis
• Preoxygenate with 100% O2
• Induce anesthesia
• Tape pt’s eyes shut to prevent corneal abrasions
• Hold laryngoscope in left hand, scissoring mouth with right thumb & index finger
→ Insert laryngoscope in right side of mouth, sweeping tongue to left
→ Advance until glottis appears in view
→ Never use laryngoscope as a lever in a pivoting motion (instead lift “up and away”)
• Using the right hand, pass the tip of the ETT through vocal cords under direct visualization
• Inflate ETT cuff with least amount of air necessary to create seal during positive-pressure ventilation
• Confirm correct placement of ETT with (1) Chest auscultation, (2) ETCO2, (3) ETT condensation, (4) palpation of ETT cuff in sternal notch
Earliest manifestation of bronchial intubation is ↑ peak pressure (right mainstem bronchus common)
• Rapid sequence intubation
• Indication: Pts at ↑ risk for aspiration (full stomach, pregnant, GERD, morbidly obese, bowel obstruction, delayed gastric emptying, pain, diabetic gastroparesis)
• Use rapid paralyzing agent: Succinylcholine (1–1.5 mg/kg) or rocuronium (0.6–1.2 mg/kg)
• Place cricoid pressure (Sellick maneuver) as pt is induced
• Protect from regurgitation of gastric contents to oropharynx
• Help visualize vocal cords during laryngoscopy
• Intubate pt once paralytic takes effect (30–60 sec); do not ventilate pt during this time
• Proper cricoid pressure should be performed with “BURP” technique:
• Displace larynx (B)ackward, (U)pward, (R)ight, with (P)ressure
• “Modified” rapid sequence intubation
• A variation of the standard RSI technique in which a mask airway is established prior to administration of a paralytic agent
• May also include use of nondepolarizing agent (pts with ↑ K+)
Ehrenfeld, JM. et al. Modified rapid sequence induction and intubation: a survey of United States current practice. Anesth Analg. 2012 Jul;115(1):95–101.
AIRWAY MANAGEMENT: NASOTRACHEAL INTUBATION
• Indications: Intraoral, facial/mandibular procedures
• Contraindications: Basilar skull fractures, nasal fractures or polyps, underlying coagulopathies
• Preparation: Anesthetize & vasoconstrict mucosa with lidocaine/phenylephrine mix or cocaine → select nares that pt can breathe through most easily
• Lubricated ETT is advanced perpendicular to face below inferior turbinate via selected nares → direct bevel laterally away from turbinates
• Advance ETT until able to visualize tip in oropharynx under direct laryngoscopy → use Magill forceps with right hand to advance/direct through vocal cords
AIRWAY MANAGEMENT: AWAKE FLEXIBLE FIBEROPTIC INTUBATION
• Equipment: Ovassapian/Willliams/Luomanen airway, topical anesthetics, vasoconstrictors, antisialagogues, suction, fiberoptic scope with lubricated ETT
• Indications: Cervical spine pathology, obesity, head & neck tumors, hx of a difficult airway
• Premedication: Sedation (midazolam, fentanyl, dexmedetomidine, ketamine)
• Technique:
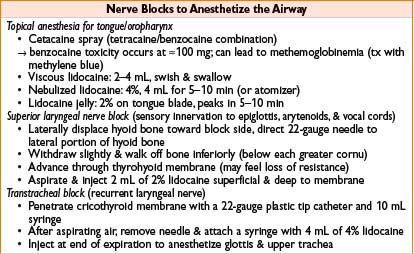
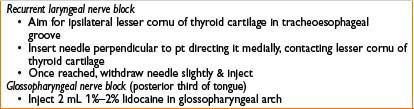
• Take time to topicalize airway (key to success; see table below)
• Place special oral airway or grab tongue with gauze
• Keep fiberoptic scope in midline while advancing until epiglottis appears
• Advance scope beneath epiglottis using antero/retroflexion as needed
• Once vocal cords are visualized, advanced scope into trachea
• Stabilized scope while ETT is advanced off scope into trachea
→ If resistance is encountered, rotate ETT tube 90 degrees
• After insertion, visualize carina with scope to avoid endobronchial intubation

TRANSTRACHEAL PROCEDURES
• Indications: Emergency tracheal access when an airway cannot be secured via nasal/oral route
• Percutaneous transtracheal jet ventilation
• Simple & relatively safe means to sustain a patient during a critical situation
• Attach 12, 14, or 16-gauge IV catheter to 10 mL syringe partially filled with saline
• Advance needle through cricothyroid membrane with constant aspiration until you get air
• Advance angiocatheter, disconnect syringe, attach oxygen source
• High-pressure O2 (25–30 psi), insufflation of 1–2 sec, 12/min with 16-gauge needle → will deliver approximately 400–700 mL
• Low-pressure O2 (bag-valve-mask 6 psi, common gas outlet 20 psi)
• Cricothyroidotomy
• Contraindications: Patients <6 yr/o (upper part of trachea not fully developed) → incision through cricothyroid membrane ↑ risk of subglottic stenosis
• Sterilize skin
• Identify cricothyroid membrane
• Transverse incision with #11 blade ≈1 cm on each side of midline
• Turn blade 90 degrees to create space to pass ETT
• Insert ETT caudally, inflate cuff, confirm breaths sounds
TECHNIQUES OF EXTUBATION
• Extubation performed when pt either deeply anesthetized (stage 3) or awake (stage 1)
• Extubation during light anesthesia (stage 2) may → laryngospasm/airway compromise
• Patient’s airway should be aggressively suctioned while on 100% O2 prior to extubation
• Prior to extubation, pt should be awake, following commands, neuromuscular blockade reversed
• Untape ETT, deflate cuff, remove ETT while providing small amount of positive pressure
• Removes secretions at distal end of ETT
• Place mask on pt with 100% O2 while verifying spontaneous & adequate ventilation
• Consider using 1.5 mg/kg of IV lidocaine 1–2 min before manipulation of airway & extubation (will blunt airway reflexes)
• Deep extubation
• Indicated to prevent ↑ BP, ICP, IOP, or bronchospasm (in asthmatics)
• Contraindicated in pts at ↑ risk for aspiration or who may have a difficult airway
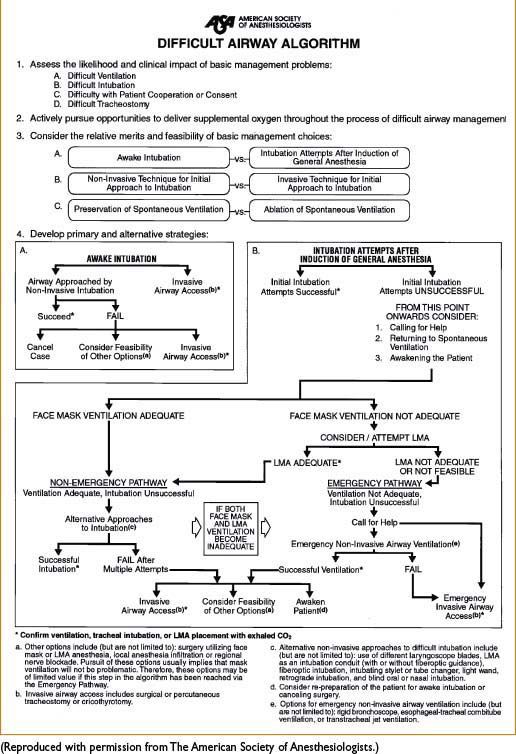
DIFFICULT AIRWAY ALGORITHM
Originally published in March 1993 & revised in 2003, the ASA Difficult Airway Algorithm (Figure 4-1) is designed to facilitate management of difficult airways & reduce adverse outcomes
Figure 4-1. ASA difficult airway algorithm. (Note: 30% of anesthesia-related deaths stem from issues of airway management.)
< div class='tao-gold-member'>









