![]() Used to obtain cerebrospinal fluid (CSF) and to measure the opening pressure of the subarachnoid space to aid in the evaluation and management of patients with acute headache or other symptoms of the following conditions:
Used to obtain cerebrospinal fluid (CSF) and to measure the opening pressure of the subarachnoid space to aid in the evaluation and management of patients with acute headache or other symptoms of the following conditions:
![]() Meningitis
Meningitis
![]() Subarachnoid hemorrhage (SAH)
Subarachnoid hemorrhage (SAH)
![]() Carcinomatous meningitis
Carcinomatous meningitis
![]() Pseudotumor cerebri (occasionally for spontaneous intracranial hypotension)
Pseudotumor cerebri (occasionally for spontaneous intracranial hypotension)
![]() Occasionally for Guillain–Barré syndrome, multiple sclerosis, inflammatory demyelinating polyneuropathy
Occasionally for Guillain–Barré syndrome, multiple sclerosis, inflammatory demyelinating polyneuropathy
![]() Occasionally in cases of encephalitis
Occasionally in cases of encephalitis
CONTRAINDICATIONS
![]() Patients who need a lumbar puncture (LP) and have any of the following should first have a brain imaging study, indicating that it is safe to perform an LP:
Patients who need a lumbar puncture (LP) and have any of the following should first have a brain imaging study, indicating that it is safe to perform an LP:
![]() Altered mental status
Altered mental status
![]() Papilledema
Papilledema
![]() New focal neurologic examination abnormalities
New focal neurologic examination abnormalities
![]() Elevated intracranial pressure (ICP)
Elevated intracranial pressure (ICP)
![]() Age 60 years or older (relative)
Age 60 years or older (relative)
![]() Immunocompromised
Immunocompromised
![]() Seizure within 1 week before presentation
Seizure within 1 week before presentation
![]() Exception, pseudotumor cerebri (where by definition, the ICP is elevated)
Exception, pseudotumor cerebri (where by definition, the ICP is elevated)
![]() Suspicion of spinal cord mass, or epidural hematoma/abscess
Suspicion of spinal cord mass, or epidural hematoma/abscess
![]() Skin or soft-tissue infection overlying lumbar spine
Skin or soft-tissue infection overlying lumbar spine
![]() Anatomic abnormalities: For example, patients with lumbar hardware from prior spinal surgery
Anatomic abnormalities: For example, patients with lumbar hardware from prior spinal surgery
![]() Coagulopathic patients
Coagulopathic patients
RISKS/CONSENT ISSUES
![]() Post-LP headache occurs in approximately 15% to 20% of patients. Using an atraumatic or noncutting spinal needle decreases the incidence of this, and multiple therapies exist to treat this specific type of headache.
Post-LP headache occurs in approximately 15% to 20% of patients. Using an atraumatic or noncutting spinal needle decreases the incidence of this, and multiple therapies exist to treat this specific type of headache.
![]() The procedure can cause local pain. Local anesthesia will be given.
The procedure can cause local pain. Local anesthesia will be given.
![]() Needle puncture can cause local bleeding, which is usually minimal
Needle puncture can cause local bleeding, which is usually minimal
![]() Potential for introducing infection exists; however, this is extremely rare. Sterile technique will be utilized.
Potential for introducing infection exists; however, this is extremely rare. Sterile technique will be utilized.
![]() Theoretical risk of damage to neural tissue exists. Such occurrences are also very rare, most often temporary, and affect spinal nerve roots, not the cord itself.
Theoretical risk of damage to neural tissue exists. Such occurrences are also very rare, most often temporary, and affect spinal nerve roots, not the cord itself.
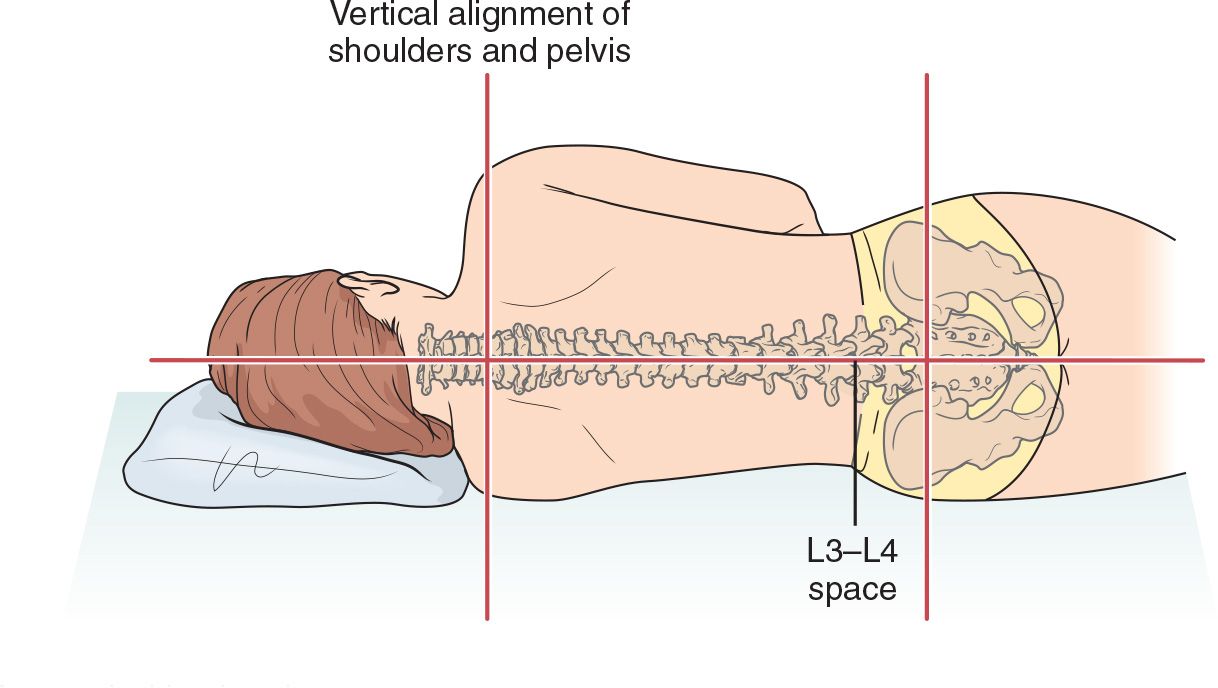
LANDMARKS
The transverse axis connecting iliac crests passes through L4 vertebral body, allowing for identification of the L4-5 and L3-4 interspaces (FIGURE 45.1)
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Explain the procedure to the patient and obtain patient consent
Explain the procedure to the patient and obtain patient consent
![]() Position the patient in either lateral decubitus or sitting position (the sitting position may be easier to use but precludes accurate ICP measurement)
Position the patient in either lateral decubitus or sitting position (the sitting position may be easier to use but precludes accurate ICP measurement)
![]() Lateral Decubitus Position
Lateral Decubitus Position
![]() Have the patient lie on one side, with knees to chest and head/shoulders curled toward knees as much as possible. Placing a pillow under the head helps reduce twisting of the shoulders.
Have the patient lie on one side, with knees to chest and head/shoulders curled toward knees as much as possible. Placing a pillow under the head helps reduce twisting of the shoulders.
![]() Ensure that the lumbar spine lies parallel to the edge of the bed. (In an infant/child, or a poorly cooperative adult, it will be necessary to have an assistant hold the patient securely in the optimal position.) The top shoulder and hip should be directly above their bottom counterparts.
Ensure that the lumbar spine lies parallel to the edge of the bed. (In an infant/child, or a poorly cooperative adult, it will be necessary to have an assistant hold the patient securely in the optimal position.) The top shoulder and hip should be directly above their bottom counterparts.
![]() A cooperative patient can be asked to curve his/her lower back, out like an “angry cat,” to optimally open the spinous processes
A cooperative patient can be asked to curve his/her lower back, out like an “angry cat,” to optimally open the spinous processes
![]() Sitting Position
Sitting Position
![]() Have the patient sit on the side of the bed with the bed positioned below patient’s midthigh and with the feet of the patient touching floor, if possible
Have the patient sit on the side of the bed with the bed positioned below patient’s midthigh and with the feet of the patient touching floor, if possible
![]() Ask the patient to curve the torso forward over a bedside table positioned in front of him/her; table height should be level with patient’s upper abdomen. A pillow may be placed on the table for patient’s comfort.
Ask the patient to curve the torso forward over a bedside table positioned in front of him/her; table height should be level with patient’s upper abdomen. A pillow may be placed on the table for patient’s comfort.
![]() After positioning, but before prepping, mark the target for needle insertion with firm pressure from the Luer-lock (hub) end of a needle sheath (or some other blunt device such as a pen) firmly against the skin (which will leave a mark for several minutes and provides a visual target)
After positioning, but before prepping, mark the target for needle insertion with firm pressure from the Luer-lock (hub) end of a needle sheath (or some other blunt device such as a pen) firmly against the skin (which will leave a mark for several minutes and provides a visual target)
![]() Prepare a wide area with povidone–iodine or chlorhexidine gluconate solution
Prepare a wide area with povidone–iodine or chlorhexidine gluconate solution
![]() Ensure the sterile field includes L4-5 and L3-4 interspaces. (Should first attempt at L4- 5 be unsuccessful, the L3-4 interspace will be readily accessible.)
Ensure the sterile field includes L4-5 and L3-4 interspaces. (Should first attempt at L4- 5 be unsuccessful, the L3-4 interspace will be readily accessible.)
![]() Use sterile drapes to frame workspace
Use sterile drapes to frame workspace
![]() Reassess landmarks. It is crucial that the midline be defined.
Reassess landmarks. It is crucial that the midline be defined.
![]() Sometimes, in overweight patients, feeling the spinous processes in the thoracic spine (where they are easier to palpate) and marching down will help the clinician ensure that they are in the midline
Sometimes, in overweight patients, feeling the spinous processes in the thoracic spine (where they are easier to palpate) and marching down will help the clinician ensure that they are in the midline
![]() Ultrasonography has been shown to reduce the failure rate, number of attempts, and traumatic punctures and can be used as an adjunct
Ultrasonography has been shown to reduce the failure rate, number of attempts, and traumatic punctures and can be used as an adjunct
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


