Inferior division of lumbar L4, L5 and sacral S1, S2, S3 nerves.
Emerges from the greater sciatic foramen.
Lies below the piriformis muscle (m.), deep to gluteus maximus m. on the posterior wall of the pelvis.
Descends between the greater trochanter of the femur and the ischial tuberosity.
Splits into the common peroneal and tibial nerves. This division may take place at any point between the sacral plexus and the lower third of the thigh.
Articular branches arise from the upper part of the nerve and supply the hip joint.
|
|
|
|


|
|
|
|
|
|



|
|
|
|
|
|
| |




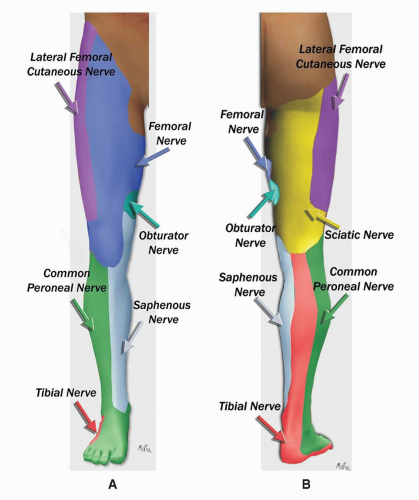
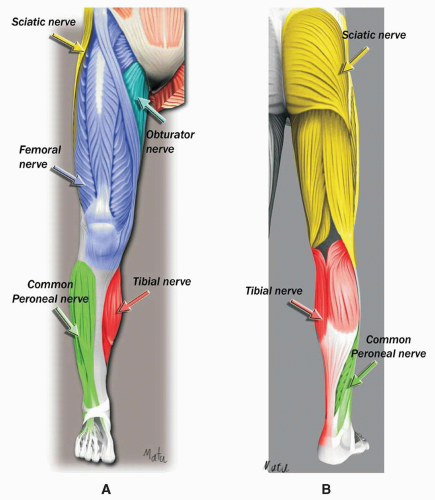
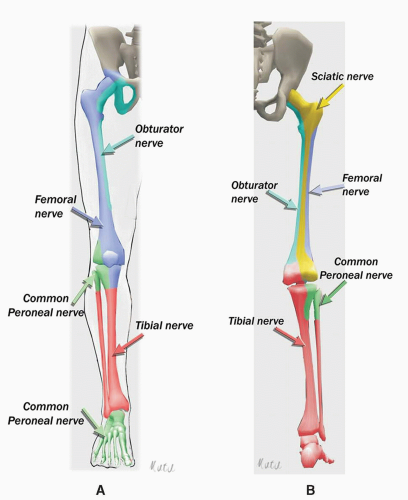
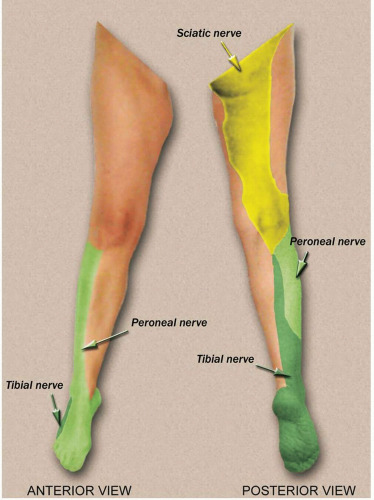 SCIATIC NERVE: DERMATOMES |
Parasacral
Classic
Lithotomy (Raj’ approach)
Subgluteal
Lateral popliteal
High posterior popliteal
Classic posterior popliteal
Line between the posterior superior iliac spine and the ischial tuberosity.
Insertion point is 6 to 7 cm caudal to the posterior superior iliac spine on this line.
Needle is introduced perpendicular to the skin or at a 30-degree angle in the cranial direction. Upon bone contact (deep landmark), the sciatic nerve is located 2 to 3 cm deeper. This bone contact corresponds to the medial part of the
greater sciatic notch of the hip bone. The needle needs to be redirected either caudally or laterally or both.
A first muscle twitch occurs when the needle is passing through the gluteus muscle. A second, deeper muscle twitch occurs when passing through the piriformis muscle. The nerve is located beneath the piriformis muscle at a depth of 6 to 9 cm.
If the first distal twitch is a hamstring contraction, deeper advancement of the needle will result in a tibial nerve stimulation (60%) or a combined tibial and common peroneal stimulation (18%).
At this level, the sciatic nerve is close to internal iliac vessels (sciatic vascular trunk).
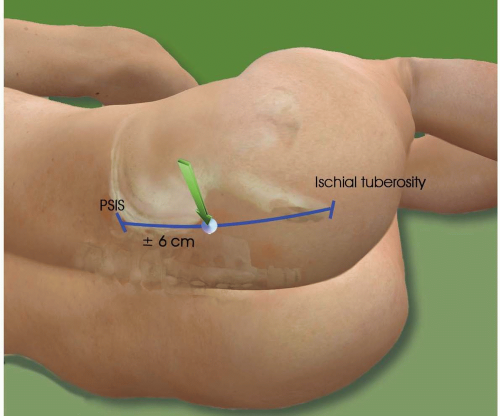 PARASACRAL APPROACH |
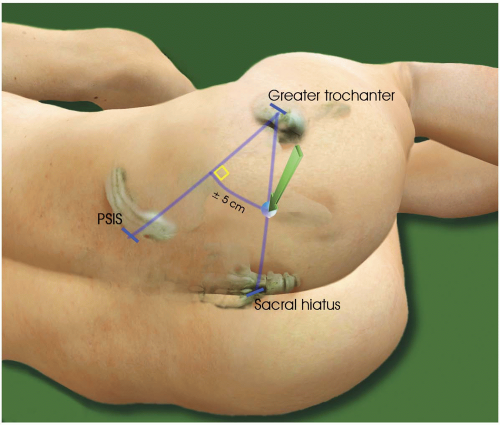
Line between the posterior superior iliac spine and the greater trochanter.
Perpendicular line is drawn at its midpoint.
Intersection with a line between the greater trochanter and the sacral hiatus. Or
5 cm on a perpendicular line drawn at the midpoint of the line between the posterior superior iliac spine and the greater trochanter.
4-inch needle.
Perpendicular to the skin.
The first contraction is elicited when the needle passes through the gluteus maximus muscle; then a deeper muscular contraction occurs when the needle passes through the piriformis muscle.
A tibial or peroneal neurostimulation is elicited 1 cm deeper.
Multistimulation: a dorsiflexion and eversion of the foot (peroneal nerve) means that the needle is stimulating the lateral part of the sciatic nerve.
A tibial n. stimulation will be elicited by moving the needle medially.
Bone contact = lateral part of the greater sciatic notch of the hip bone. The needle must be redirected medially, caudally, or both.
 CLASSIC POSTERIOR APPROACH |
Needle is introduced perpendicular to the skin.
Nerve is located at a depth of 5 to 7 cm.
Stimulation of the tibial or common peroneal nerve (hamstrings may be direct muscle stimulation).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


