(1)
Chennai Breast Centre, Chennai, India
Invasive lobular carcinoma accounts for about 10 % of all invasive carcinoma and it is the second most common breast malignancy. The unique histology of lobular carcinoma is responsible for the difficulty in early detection by mammography and accounts for high false negative detection rate in all imaging techniques.
Multifocality, multicentricity, and bilaterality (6–25 %) are common in lobular carcinomas.
Clinical Features
Classically invasive lobular carcinoma present with an area of ill-defined thickening rather than a palpable mass. Large invasive lobular cancers or the solid variants present with a palpable mass. About 40 % will have lymph nodal metastasis at presentation. Invasive lobular carcinoma has an unusual predilection to metastasize to the peritoneum, ovaries, and leptomeninges when compared to infiltrating duct carcinoma, which usually involves lung, liver, and bone.
Mammographic Features
Invasive lobular carcinoma classically grow on single file of cells without producing a desmoplastic reaction, therefore making it difficult to see on a mammogram. Even very large invasive lobular cancers can be missed on a mammogram particularly in a dense breast. Invasive lobular cancers are more likely to be diagnosed as interval cancers clinically than by screening mammography.
It is usually seen as a subtle architectural distortion or an asymmetry in one view, usually the craniocaudal view.
Less commonly lobular cancer can present as a spiculated or an ill-defined mass which is isodense with the surrounding breast structures. The extent of the disease is often underestimated on a mammogram (Figs. 32.1a, b and 32.2a, b).
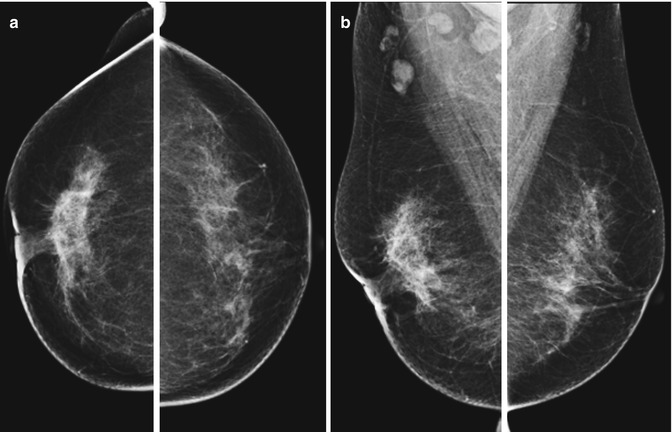
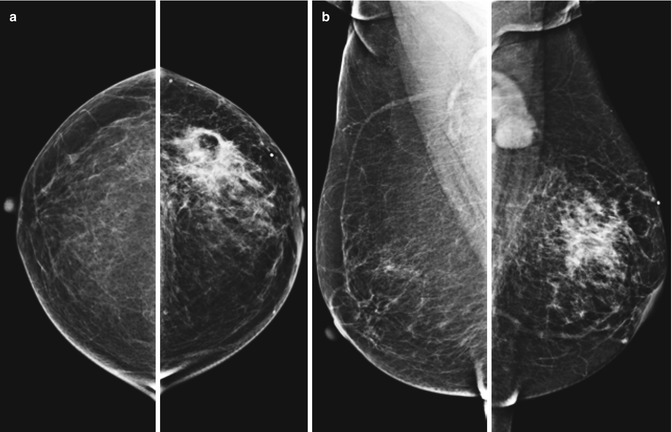
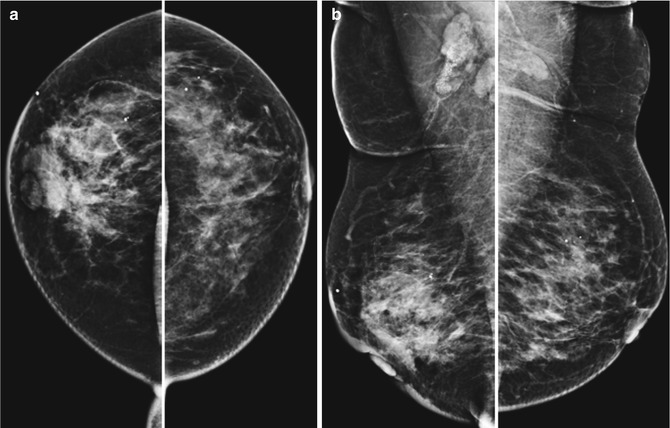
Fig. 32.1
(a, b) CC and MLO view of mammogram showing asymmetry on the right side with nipple retraction
Fig. 32.2
(a, b) CC and MLO view of mammogram showing an area of increased density in the left upper outer quadrant with enlarged axillary lymph nodes
It can produce diffuse breast change that appears like a shrinking breast on a mammogram. This is particularly evident when mammograms are compared with the previous mammograms. The sheet-like infiltrating pattern of the tumor reduces the breast’s natural elasticity, allowing for less spreading of the tissue during mammographic compression and therefore appears shrunken. Clinically, however, the breast may remain symmetric in size with respect to the other side (Fig. 32.3a, b).