Fig. 34.1
Bursas in the pelvic area
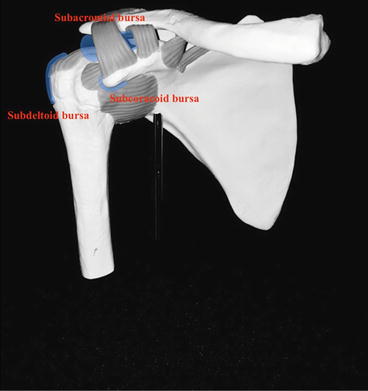
Fig. 34.2
Bursas around the shoulder
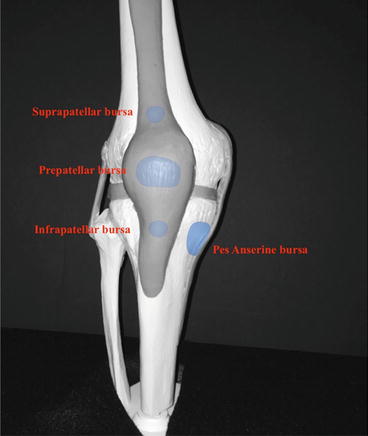
Fig. 34.3
Bursas surrounding the knee
General technique for any joint or bursa injection is relatively standard. Consent should be obtained. The patient should be positioned in a manner that would minimize injury from a potential vasovagal reaction, as well as optimizing entry into the joint space or bursa. This can usually be achieved with the patient seated or supine, depending on the target. The procedure can be performed blindly or may be guided most commonly with use of fluoroscopy or ultrasound. Aseptic technique and universal precautions are recommended to avoid introducing infection.
The type of injectate is variable. Injectate usually consists of mixture of a local anesthetic and a corticosteroid. The most common anesthetics , bupivacaine and lidocaine, temporarily leaves a joint insensate, aiding in determining a primary pain generator and may be used alone for diagnostic purposes. Corticosteroid injectates are most commonly triamcinolone and methylprednisolone and vary in half-life and solubility [5]. Hyaluronic acid is FDA-approved as an injectate for the treatment of osteoarthritis in knees. Hyaluronic acid makes up part of the molecular matrix of synovial fluid, which gives the knee viscous and elastic properties and a smooth gliding surface to help the joint move and articulate [6]. In addition, it serves to provide nutrients, remove waste products, increases lubricating ability and has anti-inflammatory properties [6, 7].
Contraindications to joint injection include bacteremia, bleeding disorder, prosthetic joint, osteochondral fracture, infectious arthritis, uncontrolled diabetes, osteomyelitis, adjacent or overlying cellulitis [8]. Post-injection care includes applying a sterile adhesive dressing over the injection site with added pressure to halt any bleeding. Icing the area 15–20 min every 4–6 h can have an analgesic response and aid in post-injection discomfort. Relative rest and avoidance of vigorous activity immediately after the injections will help prevent washout of the corticosteroid.
Related posts:
 Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
 Opioids for the Treatment of Pain in the Rehabilitation Patient
Opioids for the Treatment of Pain in the Rehabilitation Patient
 Trigeminal Neuralgia in the Rehabilitation Patient
Trigeminal Neuralgia in the Rehabilitation Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


