CHAPTER 5
Idiopathic Facial Paralysis
(Bell’s Palsy)
Presentation
The patient with this condition is often frightened by his facial disfigurement or fear of having had a stroke. He complains of a sudden onset of numbness, a feeling of fullness or swelling, periauricular pain, or some other change in sensation on one side of the face—a crooked smile, mouth “drawing,” or some other asymmetric weakness of facial muscles; an irritated, dry, or tearing eye; drooling out of the corner of the mouth; or changes in hearing or taste. Symptoms develop over several hours or days. Often there will have been a viral illness 1 to 3 weeks earlier, or there may have been another trigger, such as stress, fever, dental extraction, or cold exposure. On initial observation of the patient, it is immediately apparent that he is alert and oriented, with a partial or complete unilateral facial paralysis that includes one side of the forehead (Figure 5-1).
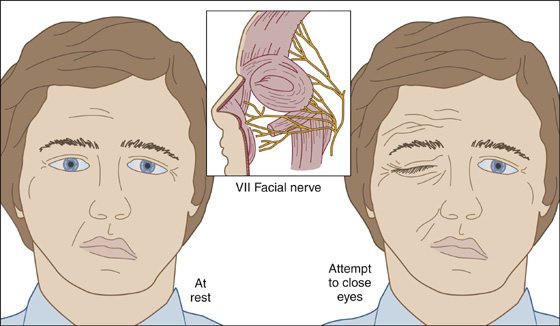
Figure 5-1 Partial or complete unilateral facial paralysis that includes one side of the forehead.
What To Do:
 Perform a thorough neurologic examination of the cranial and upper cervical nerves and limb strength, noting which nerves are involved and whether unilaterally or bilaterally. Ask the patient to wrinkle his forehead, close his eyes forcefully, smile, puff his cheeks, and whistle, observing closely for facial asymmetry. Central or cerebral lesions result in relative sparing of the forehead because of cross-innervation of the orbicularis oculi and frontalis muscles. Check tearing, ability to close the eye and protect the cornea, corneal desiccation, hearing, and, when practical, taste. Examine the ear canal and pinna for herpetic vesicles and the tympanic membrane for signs of otitis media or cholesteatoma.
Perform a thorough neurologic examination of the cranial and upper cervical nerves and limb strength, noting which nerves are involved and whether unilaterally or bilaterally. Ask the patient to wrinkle his forehead, close his eyes forcefully, smile, puff his cheeks, and whistle, observing closely for facial asymmetry. Central or cerebral lesions result in relative sparing of the forehead because of cross-innervation of the orbicularis oculi and frontalis muscles. Check tearing, ability to close the eye and protect the cornea, corneal desiccation, hearing, and, when practical, taste. Examine the ear canal and pinna for herpetic vesicles and the tympanic membrane for signs of otitis media or cholesteatoma.
 Patients with facial paralysis accompanied by acute otitis media, chronic suppurative middle-ear disease, mastoiditis, otorrhea, or otitis externa require emergent otolaryngologic consultation. Facial weakness progressing to paralysis over weeks to months, progressive twitching, or facial spasm suggests a neoplasm affecting the facial nerve. When facial paralysis is associated with pulsatile tinnitus and hearing loss, suspect a glomus tumor or cerebellar pontine angle tumor. Diplopia, dysphagia, hoarseness, facial pain, or hypesthesia suggests involvement of cranial nerves other than the seventh and calls for neurologic consultation with early magnetic resonance imaging (MRI).
Patients with facial paralysis accompanied by acute otitis media, chronic suppurative middle-ear disease, mastoiditis, otorrhea, or otitis externa require emergent otolaryngologic consultation. Facial weakness progressing to paralysis over weeks to months, progressive twitching, or facial spasm suggests a neoplasm affecting the facial nerve. When facial paralysis is associated with pulsatile tinnitus and hearing loss, suspect a glomus tumor or cerebellar pontine angle tumor. Diplopia, dysphagia, hoarseness, facial pain, or hypesthesia suggests involvement of cranial nerves other than the seventh and calls for neurologic consultation with early magnetic resonance imaging (MRI).
 If there is a history of head trauma, obtain a computed tomography (CT) scan of the head (including the skull base) or an MRI to rule out a temporal bone fracture.
If there is a history of head trauma, obtain a computed tomography (CT) scan of the head (including the skull base) or an MRI to rule out a temporal bone fracture.
 MRI with medium contrast of the skull shows a marked increase in the ability to reveal lesions, even of small dimensions, inside the temporal bone and at the cerebellopontine angle.
MRI with medium contrast of the skull shows a marked increase in the ability to reveal lesions, even of small dimensions, inside the temporal bone and at the cerebellopontine angle.
 If there are no absolute contraindications to steroid use (i.e., upper gastrointestinal [GI] bleeding, tuberculosis, acquired autoimmune deficiency syndrome [AIDS], or immunosuppression), begin therapy with prednisone, 60 mg qd, for 7 days. For patients with relative contraindications (i.e., hypertension, diabetes), consider giving prednisone in only those patients with a complete paralysis, because they are at higher risk for permanent disability. Prednisone is the only treatment shown to reduce the risk for long-term sequelae of Bell’s palsy.
If there are no absolute contraindications to steroid use (i.e., upper gastrointestinal [GI] bleeding, tuberculosis, acquired autoimmune deficiency syndrome [AIDS], or immunosuppression), begin therapy with prednisone, 60 mg qd, for 7 days. For patients with relative contraindications (i.e., hypertension, diabetes), consider giving prednisone in only those patients with a complete paralysis, because they are at higher risk for permanent disability. Prednisone is the only treatment shown to reduce the risk for long-term sequelae of Bell’s palsy.
 Although there is only controversial data to support its efficacy—but because the most widely accepted cause of a true Bell’s palsy, at present, is a neuropathy induced by herpes simplex virus—when a patient presents within 7 to 10 days of the onset of acute paresis (or paralysis) and symptoms are severe and no other cause is suspected, it is reasonable to prescribe a 10-day course of either acyclovir (Zovirax) (200 to 400 mg) 5 times per day, or 7 days of the more expensive valacyclovir (Valtrex) (1000 mg bid). There is some evidence to suggest that treatment within 3 days of the onset of symptoms with combined acyclovir and prednisone therapy may be beneficial. Again, this is most likely to have the most gain in patients with a complete lesion, because they have a higher risk for prolonged facial weakness or other sequelae.
Although there is only controversial data to support its efficacy—but because the most widely accepted cause of a true Bell’s palsy, at present, is a neuropathy induced by herpes simplex virus—when a patient presents within 7 to 10 days of the onset of acute paresis (or paralysis) and symptoms are severe and no other cause is suspected, it is reasonable to prescribe a 10-day course of either acyclovir (Zovirax) (200 to 400 mg) 5 times per day, or 7 days of the more expensive valacyclovir (Valtrex) (1000 mg bid). There is some evidence to suggest that treatment within 3 days of the onset of symptoms with combined acyclovir and prednisone therapy may be beneficial. Again, this is most likely to have the most gain in patients with a complete lesion, because they have a higher risk for prolonged facial weakness or other sequelae.
 If the cornea is dry or likely to become dry or injured as a result of the patient’s inability to produce tears and blink, protect it by patching. If patching is not necessary, recommend that the patient wear eyeglasses, apply methylcellulose artificial tears regularly during the day, and use a protective bland ointment or tape the eyelid shut at night.
If the cornea is dry or likely to become dry or injured as a result of the patient’s inability to produce tears and blink, protect it by patching. If patching is not necessary, recommend that the patient wear eyeglasses, apply methylcellulose artificial tears regularly during the day, and use a protective bland ointment or tape the eyelid shut at night.
 If the patient resides in or has traveled to a tick-endemic area, send a serum specimen for acute-phase Lyme disease titers, if available, because this is another treatable disorder that can present as a facial neuropathy. When there is a history of a tick bite or rash that is consistent with erythema migrans, a lumbar puncture may be required to make a more rapid, definitive diagnosis. In areas where Lyme disease is endemic, a 10-day course of tetracycline or doxycycline may be indicated. Amoxicillin is usually substituted for children younger than 8 years of age or for pregnant women. Cefuroxime and erythromycin have also been used successfully but are generally less effective.
If the patient resides in or has traveled to a tick-endemic area, send a serum specimen for acute-phase Lyme disease titers, if available, because this is another treatable disorder that can present as a facial neuropathy. When there is a history of a tick bite or rash that is consistent with erythema migrans, a lumbar puncture may be required to make a more rapid, definitive diagnosis. In areas where Lyme disease is endemic, a 10-day course of tetracycline or doxycycline may be indicated. Amoxicillin is usually substituted for children younger than 8 years of age or for pregnant women. Cefuroxime and erythromycin have also been used successfully but are generally less effective.
 If the cause appears to be herpes zoster-varicella or shingles of the facial nerve (e.g., grouped vesicles on the tongue), acyclovir or valacyclovir should still be effective (see Chapter 170). If the geniculate ganglion is involved (i.e., Ramsay-Hunt syndrome, with vesicles in or around the ear, decreased hearing, severe otalgia, encephalitis, meningitis), the patient may require hospitalization for IV treatment. The prognosis of Ramsay-Hunt syndrome is much worse than that of Bell’s palsy, with only 10% recovering normal function.
If the cause appears to be herpes zoster-varicella or shingles of the facial nerve (e.g., grouped vesicles on the tongue), acyclovir or valacyclovir should still be effective (see Chapter 170). If the geniculate ganglion is involved (i.e., Ramsay-Hunt syndrome, with vesicles in or around the ear, decreased hearing, severe otalgia, encephalitis, meningitis), the patient may require hospitalization for IV treatment. The prognosis of Ramsay-Hunt syndrome is much worse than that of Bell’s palsy, with only 10% recovering normal function.
 Inform the patient with uncomplicated Bell’s palsy that symptoms may progress for 7 to 10 days. Reassure him that 70% to 80% of patients with Bell’s palsy recover completely within a few weeks but that he should be aware that some patients are left with permanent facial weakness. Be aware that prognosis is linked to the severity of symptoms. Although most (94%) patients with a partial paralysis recover fully, approximately 40% with a complete paralysis at the time of presentation have some residual weakness. Provide for definite follow-up and reevaluation.
Inform the patient with uncomplicated Bell’s palsy that symptoms may progress for 7 to 10 days. Reassure him that 70% to 80% of patients with Bell’s palsy recover completely within a few weeks but that he should be aware that some patients are left with permanent facial weakness. Be aware that prognosis is linked to the severity of symptoms. Although most (94%) patients with a partial paralysis recover fully, approximately 40% with a complete paralysis at the time of presentation have some residual weakness. Provide for definite follow-up and reevaluation.
 Provide appropriate specialty referral, when there is a mass in the head or neck or a history of any malignancy.
Provide appropriate specialty referral, when there is a mass in the head or neck or a history of any malignancy.
What Not To Do:
 Do not overlook alternative causes of facial palsy that require different treatment, such as cerebrovascular accidents and cerebellopontine angle tumors (which usually produce weakness in limbs or defects of adjacent cranial nerves), multiple sclerosis (which usually is not painful, spares taste, and often produces intranuclear ophthalmoplegia), and polio (which presents as fever, headache, neck stiffness, and palsies).
Do not overlook alternative causes of facial palsy that require different treatment, such as cerebrovascular accidents and cerebellopontine angle tumors (which usually produce weakness in limbs or defects of adjacent cranial nerves), multiple sclerosis (which usually is not painful, spares taste, and often produces intranuclear ophthalmoplegia), and polio (which presents as fever, headache, neck stiffness, and palsies).
 Do not order a CT scan unless there is a history of trauma or the symptoms are atypical and include such findings as vertigo, central neurologic signs, or severe headache.
Do not order a CT scan unless there is a history of trauma or the symptoms are atypical and include such findings as vertigo, central neurologic signs, or severe headache.
 Do not make the diagnosis of Bell’s palsy in patients who report gradual onset of facial paralysis over several weeks or facial paralysis that has persisted for 3 months or more. These patients require further evaluation by a neurologist or an otolaryngologist.
Do not make the diagnosis of Bell’s palsy in patients who report gradual onset of facial paralysis over several weeks or facial paralysis that has persisted for 3 months or more. These patients require further evaluation by a neurologist or an otolaryngologist.
Discussion
Idiopathic nerve paralysis is a common malady, affecting 20 per 1 million people every year, especially diabetic or pregnant patients and those between the ages of 15 and 45 years. Up to 10% of patients have a recurrence on the same or other side of the face. The facial nerve is responsible for facial muscle innervation; lacrimal, nasal, and submandibular gland innervation; taste for the anterior two thirds of the tongue; and sensation of the external auditory canal, pinna, and tympanic membrane. Although Bell’s palsy was described classically as a pure facial nerve lesion, and physicians have tried to identify the exact level at which the nerve is compressed, the most common presenting complaints are related to trigeminal nerve involvement. The mechanism is probably a spotty demyelination of several nerves at several sites caused by reactivated herpes simplex virus. Genetic, metabolic, autoimmune, vascular, and nerve entrapment etiologies have been proposed without definitive proof. It should also be noted that for patients with Bell’s palsy, a benefit from steroids or acyclovir has not been definitively established. However, available evidence suggests that steroids are probably effective, and acyclovir (combined with prednisone) is possibly effective in improving facial functional outcomes.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


