Chapter 55
Hypothermia and Hyperthermia
Hypothermia
Clinical Manifestations
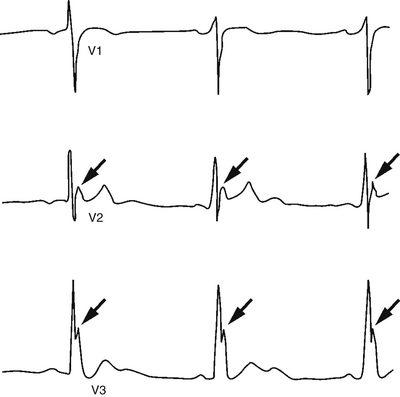
As the hypothermic patient’s compensatory mechanisms are overwhelmed, temperature-dependent physiologic changes occur. Patients with mild hypothermia demonstrate tachypnea, tachycardia, ataxia, dysarthria, impaired judgment, shivering, and diuresis. Moderate hypothermia is characterized by decreased pulse and cardiac output, hypoventilation, central nervous system depression, hyporeflexia, decreased renal blood flow, and loss of shivering. Atrial fibrillation and other arrhythmias may be seen. The electrocardiogram may manifest an Osborn or J wave (Figure 55.1); this secondary wave follows the S wave, most prominently in leads aVL, aVF, and V1–6. In severe hypothermia, coma, hypotension, pulmonary edema, oliguria, areflexia, bradycardia, ventricular arrhythmias, and asystole occur. Ventricular fibrillation is the most common fatal arrhythmia, as hypothermia lowers the heart’s fibrillation threshold. The differential diagnosis for hypothermia and predisposing factors are shown in Box 55.1.
The diagnosis of hypothermia depends on the use of a low-reading electronic thermometer to determine core temperature. It is important to know the low limit of the thermometer being used, as it is possible for the patient’s temperature to be lower than the device’s lowest reading. After making the diagnosis, laboratory evaluation should be undertaken to identify potential complications. Characteristic findings are presented in Table 55.1.
TABLE 55.1
Laboratory, Electrocardiographic, and Radiographic Findings in Hypothermia
| Tests | Findings |
| Arterial blood gas determination∗ | Metabolic acidosis, respiratory alkalosis, or both |
| Amylase determination | Increase caused by hypothermia-induced pancreatitis |
| Chest radiograph | Aspiration pneumonia, vascular congestion, pulmonary edema |
| Electrocardiogram | Prolongation of PR, QRS, QT intervals; ST segment elevations; T-wave inversions; Osborn J wave; atrial fibrillation or sinus bradycardia |
| Electrolytes | No consistent abnormality |
| Glucose | Increase, decrease, or no change |
| Hemoglobin, hematocrit | Increase caused by hemoconcentration |
| PT, PTT | Increase caused by inhibition of coagulation cascade |
| Platelet count | Decrease caused by splenic sequestration |
| WBC count | No consistent abnormality |
PT, prothrombin time; PTT, partial thromboplastin time; WBC, white blood cell.
∗Instruments routinely perform arterial blood gas analyses on samples heated to 37° C and report results as of 37° C irrespective of the patient’s temperature.
Management
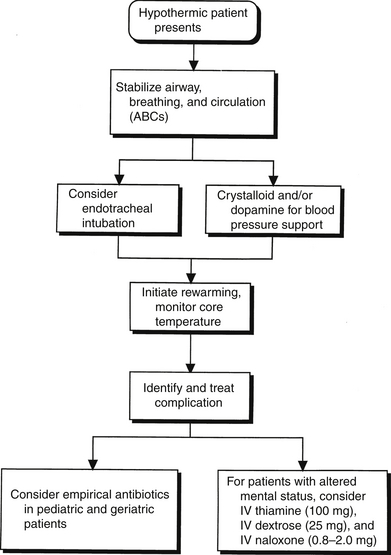
The management of hypothermia starts by stabilizing the airway, breathing, and circulation. It also includes preventing further heat loss, initiating rewarming, and treating complications (Figure 55.2). Early endotracheal intubation facilitates clearing of secretions produced by cold-induced bronchorrhea in patients with altered mental status or a decreased gag reflex. Blood pressure may be supported by crystalloid infusions. Dopamine administration should be considered in cases refractory to volume resuscitation. Core temperature should be monitored closely during therapy to prevent iatrogenic worsening of hypothermia or overshoot hyperthermia.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


