![]() Clinical suspicion of hip dislocation
Clinical suspicion of hip dislocation
![]() Hip pain with obvious deformity in the setting of a motor vehicle crash, pedestrian struck by a vehicle, falls, or sports-related injuries
Hip pain with obvious deformity in the setting of a motor vehicle crash, pedestrian struck by a vehicle, falls, or sports-related injuries
![]() Radiographic evidence of hip dislocation
Radiographic evidence of hip dislocation
CONTRAINDICATIONS
![]() Associated femoral neck fracture
Associated femoral neck fracture
![]() Coexistent fracture in dislocated extremity
Coexistent fracture in dislocated extremity
RISKS/CONSENT ISSUES
![]() Inadvertently converting a dislocation to a fracture-dislocation (acetabulum or femoral head fracture)
Inadvertently converting a dislocation to a fracture-dislocation (acetabulum or femoral head fracture)
![]() More common in the elderly with osteoporotic bones
More common in the elderly with osteoporotic bones
![]() Oversedation may lead to inability to protect the airway with subsequent potential risk of aspiration
Oversedation may lead to inability to protect the airway with subsequent potential risk of aspiration
![]() General Basic Steps
General Basic Steps
![]() Obtain radiographs
Obtain radiographs
![]() Sedation/Analgesia
Sedation/Analgesia
![]() Have assistants for help
Have assistants for help
![]() Perform procedure
Perform procedure
LANDMARKS
![]() Posterior Hip Dislocation
Posterior Hip Dislocation
![]() Mechanism of injury—femoral head is forced out of the acetabulum and rests posteriorly
Mechanism of injury—femoral head is forced out of the acetabulum and rests posteriorly
![]() Clinical features—affected extremity shortened, adducted, and internally rotated; patient may hold hip flexed with knee of affected extremity resting on opposite knee (FIGURE 66.1)
Clinical features—affected extremity shortened, adducted, and internally rotated; patient may hold hip flexed with knee of affected extremity resting on opposite knee (FIGURE 66.1)
![]() Radiographic evidence—femoral head resting posterior to the acetabulum (FIGURE 66.2)
Radiographic evidence—femoral head resting posterior to the acetabulum (FIGURE 66.2)
![]() Anterior Hip Dislocation
Anterior Hip Dislocation
![]() Mechanism—forced abduction with the hip in a flexed position or forced hyperextension of the hip
Mechanism—forced abduction with the hip in a flexed position or forced hyperextension of the hip
![]() Clinical features—affected extremity abducted, slight flexion, and externally rotated
Clinical features—affected extremity abducted, slight flexion, and externally rotated
![]() Radiographic evidence—femoral head dislocated medially toward obturator foramen (obturator dislocation) and femoral head dislocated laterally toward pubis (pubic dislocation) (FIGURE 66.3)
Radiographic evidence—femoral head dislocated medially toward obturator foramen (obturator dislocation) and femoral head dislocated laterally toward pubis (pubic dislocation) (FIGURE 66.3)
TECHNIQUE
![]() Preprocedure
Preprocedure
![]() Radiographs
Radiographs
![]() Should be obtained preprocedure only if there is a concern for a fracture or to determine the position of the dislocation
Should be obtained preprocedure only if there is a concern for a fracture or to determine the position of the dislocation
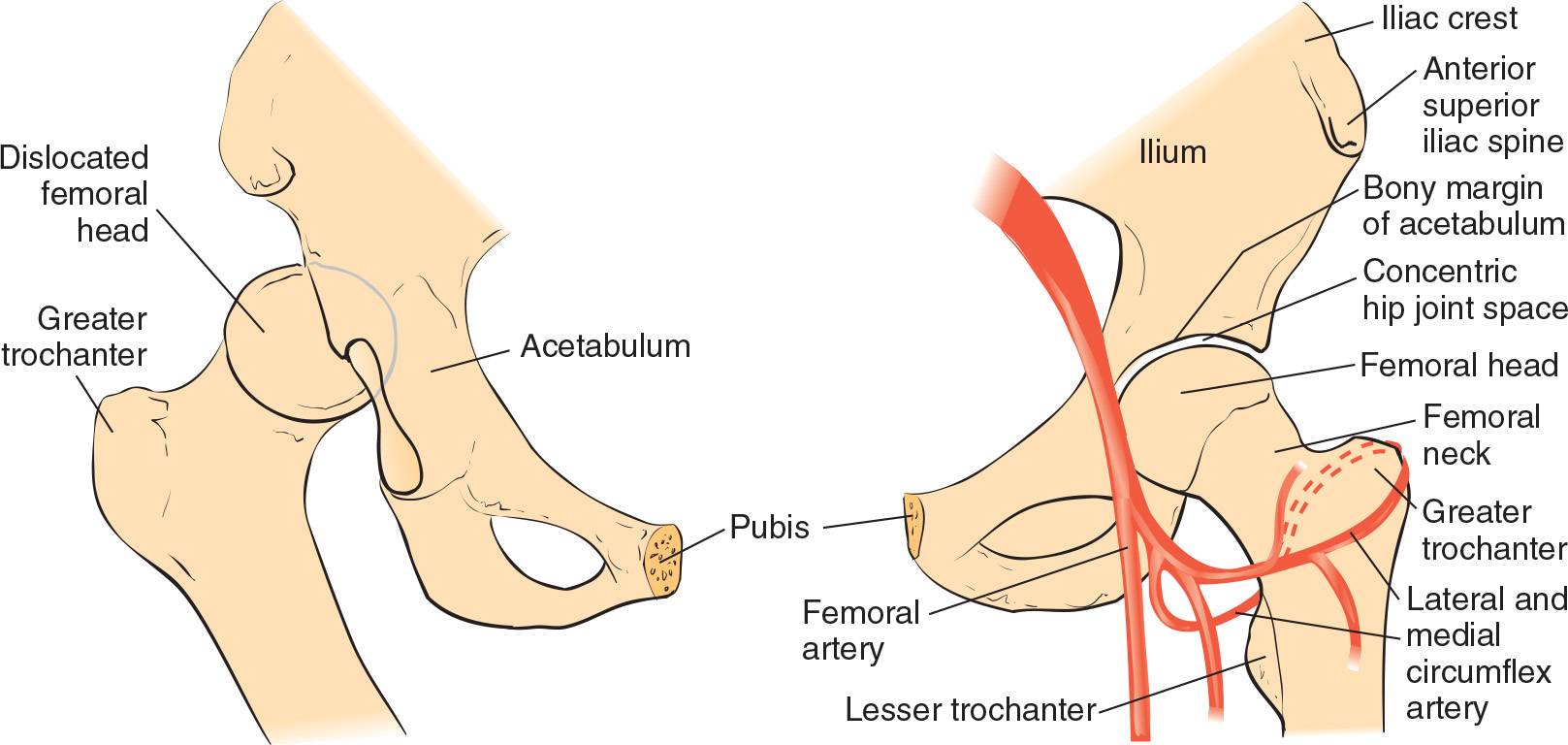
FIGURE 66.1 Normal (left) and dislocated (right) hip. (From Young GM. Reduction of common joint dislocations and subluxations. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:1093, with permission.)
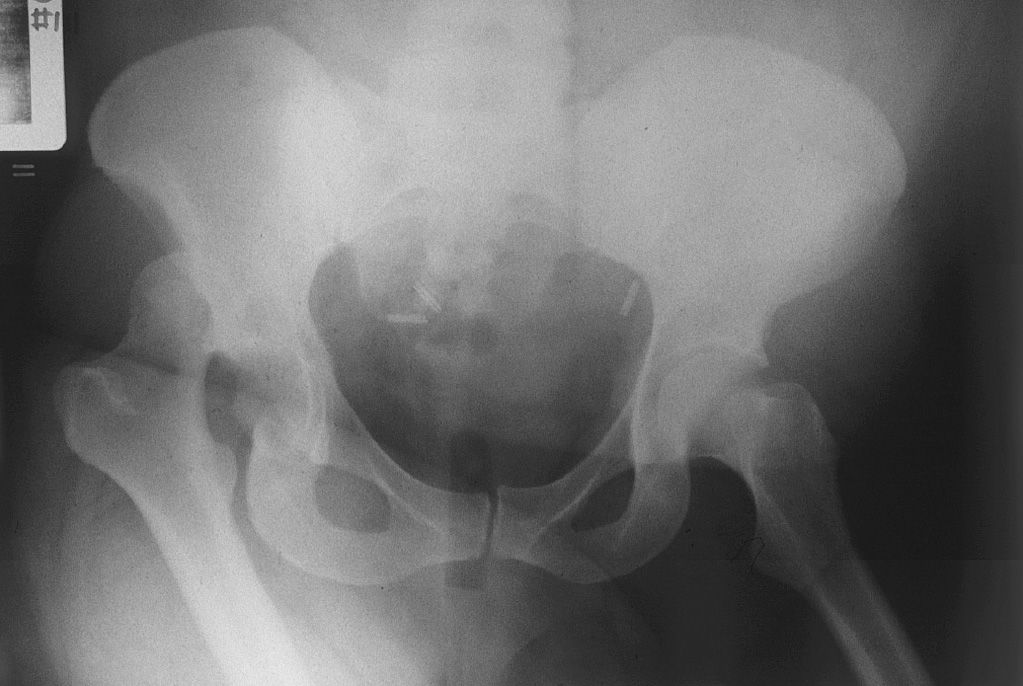
FIGURE 66.2 Anteroposterior pelvis radiograph of a posterior hip dislocation of the right hip. (From Tornetta Paul III. Hip dislocations and fractures of the femoral head. In: Bucholz RW, Heckman JD, Court-Brown C, eds. Rockwood and Green’s Fractures in Adults. Vol 2. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:1718, with permission.)
![]() Posterior Dislocation Reduction
Posterior Dislocation Reduction
![]() Allis Maneuver (FIGURE 66.4)
Allis Maneuver (FIGURE 66.4)
![]() Patient is placed supine
Patient is placed supine
![]() Downward stabilization of the pelvis is performed by an assistant
Downward stabilization of the pelvis is performed by an assistant
![]() With the knee flexed, apply traction in-line with the deformity with gentle flexion of the hip to 90 degrees
With the knee flexed, apply traction in-line with the deformity with gentle flexion of the hip to 90 degrees
![]() Perform gentle internal-to-external rotation as the hip is flexed
Perform gentle internal-to-external rotation as the hip is flexed
![]() Once reduction is achieved, hip is brought to the extended position while traction is maintained
Once reduction is achieved, hip is brought to the extended position while traction is maintained
![]() Legs are then immobilized in slight abduction through the placement of pillows between the knees
Legs are then immobilized in slight abduction through the placement of pillows between the knees

FIGURE 66.3 Anteroposterior pelvis radiograph of an anterior hip dislocation of the left hip. (From Tornetta Paul III. Hip dislocations and fractures of the femoral head. In: Bucholz RW, Heckman JD, Court-Brown C, eds. Rockwood and Green’s Fractures in Adults. Vol 2. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:1720, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


