Head Blocks
A. A.J. Maillard
Historically, the best-known major surgical procedure of the head performed under regional anesthesia in the United States is the partial maxillectomy performed on President Grover Cleveland in 1893. This chapter is presented according to the anatomic sites and types of nerves (scalp and face, facial nerves, trigeminal nerve, midface, and mandibular nerve). For each site, the relevant anatomy and the corresponding blocks will be described. Since most head blocks involve cranial nerves or their branches, consideration will also be given to the bony anatomy and especially the neural foramina. All of these blocks can be performed with the patient in the sitting or supine position depending on the block and the condition of the patient.
A. Blocks of the Scalp and Face
Originally, these blocks were directed at specific cutaneous nerves to block their sensory distribution. However, as epinephrine came into general use, its hemostatic effects on the scalp became a great aid to neurosurgeons. Therefore, instead of electively blocking these nerves, surgeons started to infiltrate the scalp around their proposed incision sites.
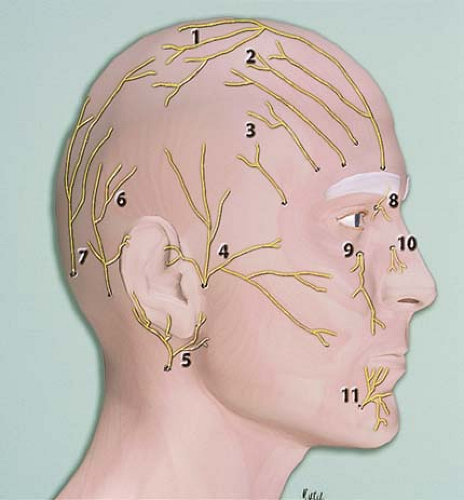 Figure 23-1. Cutaneous nerves supplying the scalp and face. |
B. Blocks of the Facial Nerve
The combination of a supraorbital nerve block and an infraorbital nerve block provides complete anesthesia of the periorbita (Fig. 23-2).
The advantages of this technique over infiltrating techniques are that the volume of the soft tissues is not augmented by these injections and that there is no soft tissue distortion. Therefore, the surgeon has much better perspective to plan and carry out the repairs.
 Figure 23-2. The combination of a supraorbital nerve block and an infraorbital nerve block provides complete anesthesia of the periorbita. |
C. Blocks of the Trigeminal Nerve and Associated Dermatomes for V1, V2, and V3
The first division of the trigeminal nerve (V1) gives rise to the supraorbital nerve, which exits the brain through the supraorbital fissure. This branch gives sensation to the forehead and parietal scalp. The second division (V2) exits through the infraorbital fissure to exit into the face through the infraorbital foramen, located at approximately the midpoint of the infraorbital rim. Figure 23-3 depicts the cutaneous dermatomes associated with the different sensory branches of the trigeminal nerve.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


