![]() For acute compartment syndrome treatment (TABLE 53.1)
For acute compartment syndrome treatment (TABLE 53.1)
![]() Common locations for compartment syndrome include the calf, the anterior thigh, and the forearm
Common locations for compartment syndrome include the calf, the anterior thigh, and the forearm
![]() Once the diagnosis is made, early fasciotomy is advocated to reduce the risk of limb loss or dysfunction, rhabdomyolysis, lactic acidosis, and infection
Once the diagnosis is made, early fasciotomy is advocated to reduce the risk of limb loss or dysfunction, rhabdomyolysis, lactic acidosis, and infection
![]() Muscle death typically begins within 4 to 6 hours of vascular compromise; irreversible damage is usually achieved by 12 hours
Muscle death typically begins within 4 to 6 hours of vascular compromise; irreversible damage is usually achieved by 12 hours
![]() Early consultation should be obtained with general, vascular, and/or orthopedic surgery
Early consultation should be obtained with general, vascular, and/or orthopedic surgery
CONTRAINDICATIONS
![]() Although there are no absolute contraindications to fasciotomy in the acute setting, relative contraindications may include:
Although there are no absolute contraindications to fasciotomy in the acute setting, relative contraindications may include:
![]() A nonviable extremity
A nonviable extremity
![]() Acute compartment syndrome associated with snake bites
Acute compartment syndrome associated with snake bites
RISKS/CONSENT ISSUES
![]() Pain
Pain
![]() Bleeding
Bleeding
![]() Infection
Infection
![]() Iatrogenic injury to nerve, muscle, and vascular structures
Iatrogenic injury to nerve, muscle, and vascular structures
![]() Continued muscle damage, despite intervention
Continued muscle damage, despite intervention
![]() General Basic Steps
General Basic Steps
![]() Conscious sedation and analgesia
Conscious sedation and analgesia
![]() Sterilization
Sterilization
![]() Fasciotomy
Fasciotomy
![]() Verification
Verification
EXTERNAL AND INTERNAL CAUSES OF COMPARTMENT SYNDROME |
External causes | Internal causes |
|
|
Adapted from Moore EE. Trauma. 5th ed. New York, NY: McGraw Hill; 2005:903; table 41-1. | |
LANDMARKS
![]() The forearm—there are two compartments
The forearm—there are two compartments
![]() The volar compartment of the arm is accessed through a volar–ulnar incision beginning 3 cm below the medial epicondyle and running down the volar–ulnar aspect of the arm, ending 5 cm proximal to the ulnar styloid. This incision allows for soft-tissue coverage of the flexor tendons and ulnar and median nerves (FIGURES 53.1 and 53.2).
The volar compartment of the arm is accessed through a volar–ulnar incision beginning 3 cm below the medial epicondyle and running down the volar–ulnar aspect of the arm, ending 5 cm proximal to the ulnar styloid. This incision allows for soft-tissue coverage of the flexor tendons and ulnar and median nerves (FIGURES 53.1 and 53.2).
![]() The dorsal compartment of the arm is accessed through a dorsal incision from 2 cm below the lateral epicondyle, cutting longitudinally to the midline of the dorsum of the wrist
The dorsal compartment of the arm is accessed through a dorsal incision from 2 cm below the lateral epicondyle, cutting longitudinally to the midline of the dorsum of the wrist
![]() The lower leg—there are four compartments accessible by two approaches
The lower leg—there are four compartments accessible by two approaches
![]() Double-incision fasciotomy; two approximately 8-cm incisions are made
Double-incision fasciotomy; two approximately 8-cm incisions are made
![]() Lateral incision 1 cm anterior to the fibula
Lateral incision 1 cm anterior to the fibula
![]() Begin 2 cm below the fibular head and continue two-thirds of the length of the leg—this avoids peroneal nerve where it exits the fascia
Begin 2 cm below the fibular head and continue two-thirds of the length of the leg—this avoids peroneal nerve where it exits the fascia
![]() Make two corresponding fascial incisions; one into the anterior compartment and one into the lateral compartment (FIGURE 53.3)
Make two corresponding fascial incisions; one into the anterior compartment and one into the lateral compartment (FIGURE 53.3)
![]() Medial incision 2 cm posterior to the tibia; stay posterior incising over the gastrocnemius
Medial incision 2 cm posterior to the tibia; stay posterior incising over the gastrocnemius
![]() Begin 2 cm below the tibial tuberosity and continue two-thirds the length of the leg—this course avoids the saphenous vein and nerve
Begin 2 cm below the tibial tuberosity and continue two-thirds the length of the leg—this course avoids the saphenous vein and nerve
![]() Make two corresponding fascial incisions; one into the superficial posterior compartment and other into the deep posterior compartment
Make two corresponding fascial incisions; one into the superficial posterior compartment and other into the deep posterior compartment
![]() The perifibular approach has been shown to be less efficacious, requires more exposure, may require fibulectomy, and has generally fallen out of favor
The perifibular approach has been shown to be less efficacious, requires more exposure, may require fibulectomy, and has generally fallen out of favor
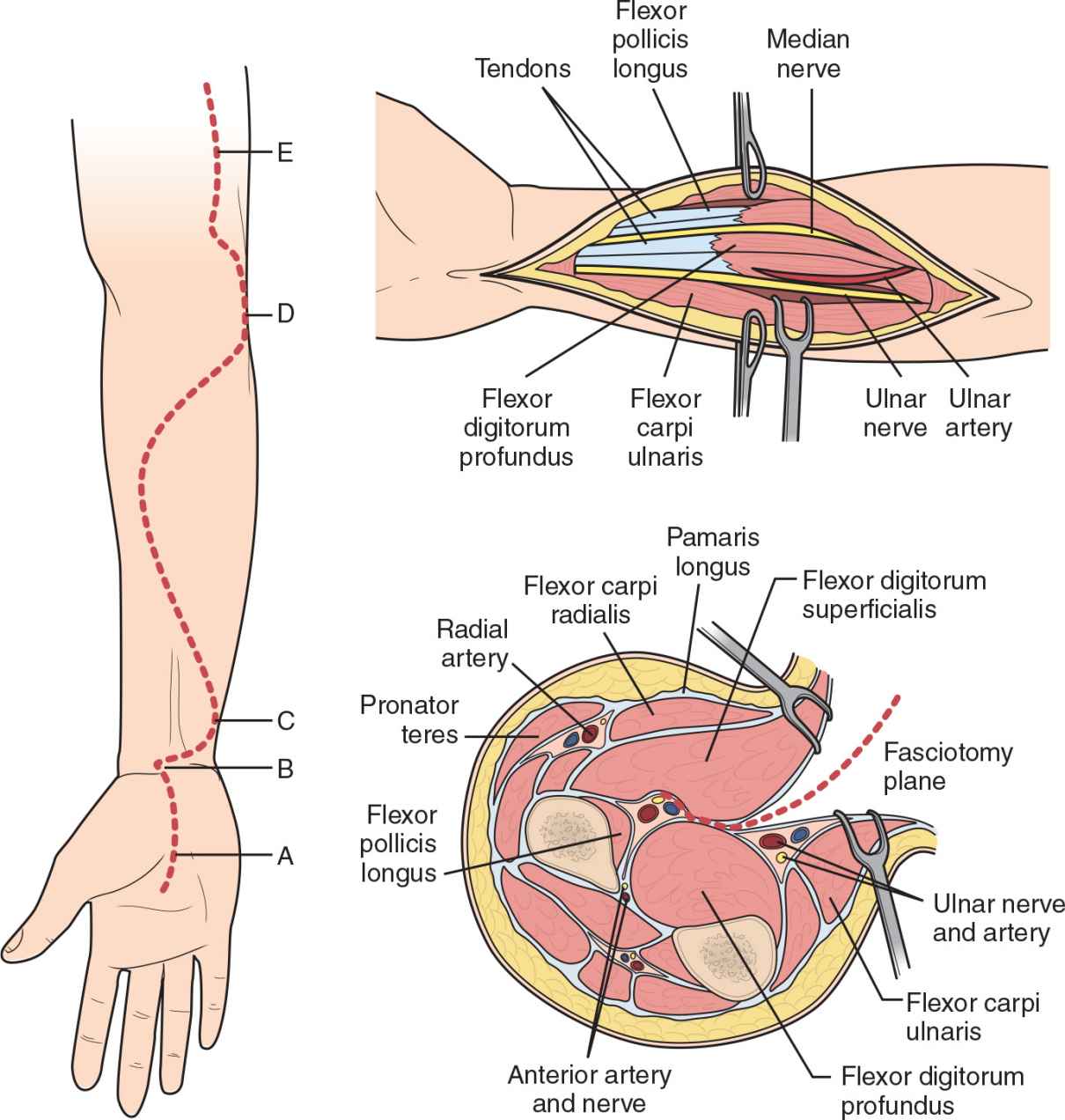
FIGURE 53.1 Volar release in the forearm. The upper illustration shows the incision that is used. The lower left picture depicts the relevant incisional anatomy. The lower right picture depicts the cross-sectional anatomy.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


