76 Facial Trauma
 Key Points
Key Points• Treatment of all facial injuries should initially be directed toward maintaining the airway and stabilizing life-threatening injuries.
• Facial computed tomography is routinely performed to visualize facial fractures; however, plain radiographs may be sufficient in patients with isolated facial injury and a low index of suspicion for a midface fracture or concomitant intracranial injuries.
Perspective
A person’s face is the focal point of conversation and social interaction. Within the face is embodied each person’s mode of expression and communication. The face also has a receptive importance, with many special sensory functions of the body located within the facial structures. It is not surprising that facial disfigurement harbors the potential for both physical impairment and long-term psychologic sequelae.1,2
Death from facial trauma is rare, and the severity of facial injuries is often perceived by the patient to be out of proportion to the actual injury. The goal of the emergency physician (EP) is to secure the airway, identify the injury, preserve appearance, and consult with the appropriate surgeon to determine further treatment and follow-up.3 Although zygomatic and nasal fractures may occur in isolation, any fracture of the frontal bone and maxilla must raise suspicion for the possibility of associated facial fractures, intracranial injury, and concomitant cervical spine injury.4–7 Proper diagnosis and recognition of zygoma and nasal pathology are essential for maintenance of adequate cosmetic and physiologic function. Trauma involving the mandible, the strongest facial bone, may result in fracture or dislocation. Fifty percent of mandibular fractures occur at two or more locations because of its pseudo-ring shape. Detection of one fracture site should always prompt a search for a second fracture.8
General Anatomy
The major bones of the face create the defining features and include the frontal, nasal, zygoma, maxilla, mandible, and temporal bones. The orbit consists of the maxilla, zygoma, frontal, sphenoid, orbital, and lacrimal bones (Fig. 76.1).
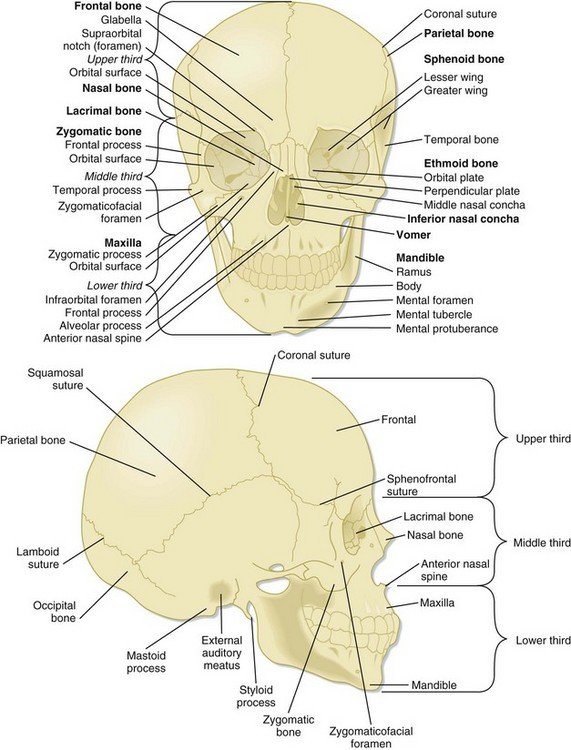
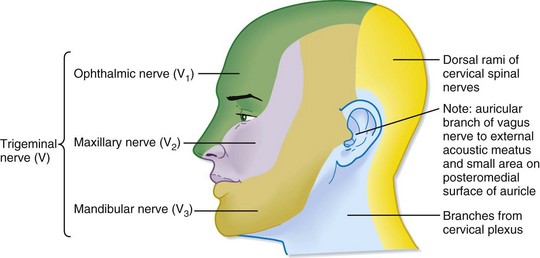
The face is conventionally divided into thirds: upper, middle, and lower. The borders of each third are loosely defined by branches of the trigeminal nerve, which provides sensory innervation to the face. Identification of the exiting foramen for the distributing branches of the trigeminal nerve (cranial nerve V) is crucial when providing local nerve anesthesia (Fig. 76.2).
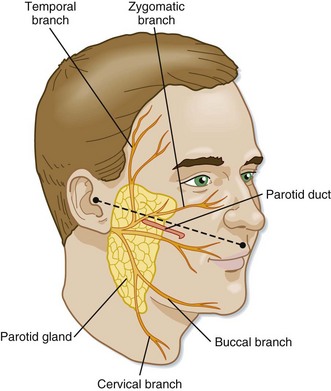
The parotid duct lies in a plane with the tragus and inferior corner of the nasal vestibule. Competency of the parotid duct must be considered in patients with deep lacerations in this region of the face (Fig. 76.3).9
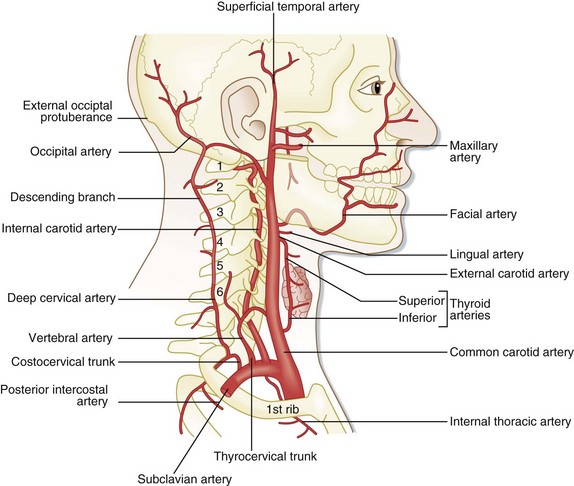
The external carotid artery is the major vascular supply to the face. This vessel provides extensive collateral supply to the midline tissues through anastomosis (Fig. 76.4).10
Approach to Multitrauma Patients with Facial Injuries
The degree of tissue distortion following facial trauma should not dissuade the EP from addressing the initial treatment priorities in patients. Though uncommon, facial trauma can be a life-threatening insult, and the EP must address life-threatening injuries before evaluating the obvious facial injury. The mere presence of a facial fracture, particularly one involving the midface, greatly increases the risk for traumatic brain injury.11,12 The energy required to fracture the midface is often transmitted to the neurocranium, and such fractures are associated with a high incidence of brain death. In general, patients with facial fractures who do not survive have higher injury severity scores and lower Glasgow Coma Scale scores and consist of an older population. Other typical concomitant injuries include pulmonary contusions, abdominal injuries, and cervical spine injuries.13 The emergence of motor vehicle air bags has decreased patient mortality. However, increased concern is warranted for injuries to the orbits, globes, facial soft tissues, and temporomandibular joints, as well as cervical fractures of the posterior arches of C1 and C2.
Treatment of bleeding must begin with inspection of the airway and maintenance of its patency. Local hemorrhage may be controlled with posterior nasal packing or insertion of a Foley catheter into the nasopharynx and inflation with air. The catheter should be gently pulled anteriorly in an attempt to close the posterior choana. Temporary external reduction of fractures may also provide stabilization of arterial injuries. Finally, surgical ligation of the external carotid artery or transcatheter arterial embolization of the maxillary artery can be performed to effect hemostasis.14 Less obvious sources of serious blood loss must be monitored (scalp lacerations, nasal fractures, mandibular fractures) because persistent bleeding may lead to hypovolemia.15
Frontal Skull Injuries
Treatment
Frontal sinus fractures are usually diagnosed by computed tomography (CT). Displaced anterior wall fractures require either immediate repair or delayed reconstruction. Conversely, frontal bone fractures that involve the posterior wall of the sinus are associated with cerebrospinal fluid (CSF) rhinorrhea; the patient will require urgent consultation with a neurosurgeon and admission to the hospital.16 Ocular trauma or sudden loss of vision associated with a frontal bone injury requires immediate ophthalmologic consultation.
Blunt Ophthalmic and Orbital Trauma
Pathophysiology
Trauma to the eye can result from falls, motor vehicle accidents, and direct blows from an assault or a projectile object (hockey puck, baseball). Serious eye injury has been shown to most commonly be associated with midface fractures.17,18 Ocular trauma can be divided into two broad categories: direct trauma to the globe and trauma to the orbit. Direct globe trauma ranges in severity from a benign corneal abrasion to rupture of the globe. Orbital trauma involves injuries such as benign contusions and fractures with complications to surrounding structures, including the globe and extraocular muscles.
Orbital fractures are classified as “impure” when the fracture line involves the orbital rim or as “pure” in the case of a fracture with no rim involvement. Compression of the optic nerve (ocular neuropathy) can be caused by displacement of a fracture, increased pressure from a retrobulbar hemorrhage, or optic nerve hemorrhage.19 Each of these processes has the potential to lead to rapidly progressive visual loss and is an ophthalmologic emergency.
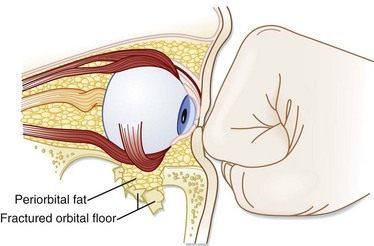
The mechanism of orbital blowout fractures was investigated by Waterhouse et al. via the same principles as Le Fort a century earlier (see later).20 Waterhouse investigated the two possible mechanisms for an orbital blowout fracture, the hydraulic and buckling theories. The hydraulic mechanism occurs when the vector of the force directed onto an uninjured globe is transmitted to the fixed orbital walls; it results in a large fracture of the inferior or medial orbital wall, or both (Fig. 76.5). This mechanism is commonly associated with herniation of the orbital contents through the fractured orbital wall, hence the term blowout. The buckling mechanism, in contrast, occurs when a traumatic force is directed to the inferior orbital rim and causes only the inferior floor of the orbit to buckle, or fracture, with no associated herniation of the orbital contents.
Presenting Signs and Symptoms
Key points in the patient’s history include the following:
• Binocular diplopia (blurring of vision when both eyes are open) is indicative of an ocular muscle imbalance between the two eyes as a consequence of muscle entrapment, contusion, or displacement of the globe secondary to edema from surrounding structures.
• Monocular diplopia (blurring of vision when only one eye is open) is often indicative of lens dislocation, hyphema, or partial globe rupture.
• Flashing lights, or floaters, can be consistent with a retinal tear, retinal detachment, or vitreous hemorrhage.
• Any loss of perception of light or identification of colors or the presence of central scotomata without association with pain is indicative of optic neuropathy. Absence of light perception following an orbital fracture is a poor prognostic indicator for recovery of vision.
• Rapid loss of vision in one eye associated with edema, proptosis, and tension on palpation should heighten suspicion for the presence of a retrobulbar hematoma.
• Pain with eye movement is commonly associated with an orbital fracture.
Treatment
Management of blowout fractures is complicated.21 The presence of an orbital fracture with findings of herniation on clinical or radiographic examination requires immediate surgical consultation to guide the treatment plan. Immediate indications for surgical intervention include muscular entrapment with gaze restriction or acute enophthalmos. Contraindications to surgery include globe rupture, hyphema, and retinal tears. These injuries should prompt emergency ophthalmologic consultation. An ophthalmologist should also be contacted for patients with evidence of lens dislocation, laceration of the cornea or sclera, or rapid loss of visual acuity.







