Nasal bleeding that does not stop with a topical vasoconstrictor and direct pressure applied by the patient (described below in the “Technique” section).
PROCEDURES
![]() Cauterization
Cauterization
![]() Anterior source bleeding that can be visualized
Anterior source bleeding that can be visualized
![]() Anterior Nasal Packing
Anterior Nasal Packing
![]() Anterior source bleeding that cannot be visualized
Anterior source bleeding that cannot be visualized
![]() Cauterization fails
Cauterization fails
![]() Posterior Nasal Packing or Balloon Tamponade
Posterior Nasal Packing or Balloon Tamponade
![]() Anterior source cannot be identified and
Anterior source cannot be identified and
![]() Bleeding from both nares or
Bleeding from both nares or
![]() Blood draining into the posterior pharynx
Blood draining into the posterior pharynx
![]() Anterior packing of both nares fails to control bleeding
Anterior packing of both nares fails to control bleeding
CONTRAINDICATIONS
![]() None
None
RISKS
![]() Nasal packing can cause pain or discomfort
Nasal packing can cause pain or discomfort
![]() Risk of infection, septal damage, and ulceration
Risk of infection, septal damage, and ulceration
![]() Risk of balloon migration, airway obstruction, or aspiration with posterior packing
Risk of balloon migration, airway obstruction, or aspiration with posterior packing
LANDMARKS
![]() The choice of procedure depends on the source of bleeding. The source can be identified by direct visualization, or with use of a nasal speculum (described in more detail in the “Technique” section).
The choice of procedure depends on the source of bleeding. The source can be identified by direct visualization, or with use of a nasal speculum (described in more detail in the “Technique” section).
![]() Nosebleeds are most commonly anterior (80% to 90%), originating from the Kiesselbach plexus in the septum
Nosebleeds are most commonly anterior (80% to 90%), originating from the Kiesselbach plexus in the septum
![]() Most posterior nosebleeds originate from branches of the sphenopalatine artery in the posterior nasal cavity or nasopharynx. A posterior source is likely when an anterior source cannot be identified, when bleeding is from both nares, or when blood is draining into the posterior pharynx.
Most posterior nosebleeds originate from branches of the sphenopalatine artery in the posterior nasal cavity or nasopharynx. A posterior source is likely when an anterior source cannot be identified, when bleeding is from both nares, or when blood is draining into the posterior pharynx.
![]() General Basic Steps
General Basic Steps
![]() Patient preparation
Patient preparation
![]() Analgesia
Analgesia
![]() Visualization
Visualization
![]() Cauterization
Cauterization
![]() Anterior packing
Anterior packing
![]() Posterior packing
Posterior packing
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Ask the patient to blow his or her nose, which decreases the effects of local fibrinolysis and removes clots (FIGURE 75.1)
Ask the patient to blow his or her nose, which decreases the effects of local fibrinolysis and removes clots (FIGURE 75.1)
![]() Ask the patient to lean forward and apply continuous pressure to the alae of both nares for 10 to 20 minutes. If this stops bleeding, consider sending patient home with follow-up to ear, nose, and throat (ENT) specialist or Primary Medical Doctor (PMD).
Ask the patient to lean forward and apply continuous pressure to the alae of both nares for 10 to 20 minutes. If this stops bleeding, consider sending patient home with follow-up to ear, nose, and throat (ENT) specialist or Primary Medical Doctor (PMD).
![]() Analgesia
Analgesia
![]() Apply a topical anesthetic and vasoconstrictor
Apply a topical anesthetic and vasoconstrictor
![]() Soak cotton or gauze in 2% lidocaine with or without topical epinephrine or 4% topical cocaine. Place in the nasal cavity for 15 to 20 minutes.
Soak cotton or gauze in 2% lidocaine with or without topical epinephrine or 4% topical cocaine. Place in the nasal cavity for 15 to 20 minutes.
![]() Alternatively, a topical anesthetic with a decongestant (2% lidocaine and 4% phenylephrine mixed 1:1) or oxymetazoline hydrochloride (Afrin) nasal spray may be used
Alternatively, a topical anesthetic with a decongestant (2% lidocaine and 4% phenylephrine mixed 1:1) or oxymetazoline hydrochloride (Afrin) nasal spray may be used
![]() Because patients may be apprehensive and packing is uncomfortable, opiates or benzodiazepines may be given before the examination (strongly recommended in cases of posterior packing)
Because patients may be apprehensive and packing is uncomfortable, opiates or benzodiazepines may be given before the examination (strongly recommended in cases of posterior packing)
![]() Visualization
Visualization
![]() Position the patient sitting upright, facing forward in the sniffing position
Position the patient sitting upright, facing forward in the sniffing position
![]() Insert a nasal speculum so that one blade moves superiorly and the other inferiorly and spread the nares vertically. Suction all remaining clots and blood. This permits visualization of most anterior sources.
Insert a nasal speculum so that one blade moves superiorly and the other inferiorly and spread the nares vertically. Suction all remaining clots and blood. This permits visualization of most anterior sources.
![]() Cauterization
Cauterization
![]() If an anterior source is visualized, cauterization should be attempted. To be effective, cautery should be performed after bleeding is controlled. Only cauterize one side of the septum at a time to prevent perforation or necrosis of the septum.
If an anterior source is visualized, cauterization should be attempted. To be effective, cautery should be performed after bleeding is controlled. Only cauterize one side of the septum at a time to prevent perforation or necrosis of the septum.
![]() Chemical cauterization can be performed using silver nitrate sticks. Apply the tip of a silver nitrate stick to the bleeding site until a white precipitate forms (usually a few seconds, rarely more than 10).
Chemical cauterization can be performed using silver nitrate sticks. Apply the tip of a silver nitrate stick to the bleeding site until a white precipitate forms (usually a few seconds, rarely more than 10).
![]() If bleeding is vigorous, electrocauterization can be used. Apply the device to the bleeding site for up to 10 seconds or until a white precipitate forms.
If bleeding is vigorous, electrocauterization can be used. Apply the device to the bleeding site for up to 10 seconds or until a white precipitate forms.
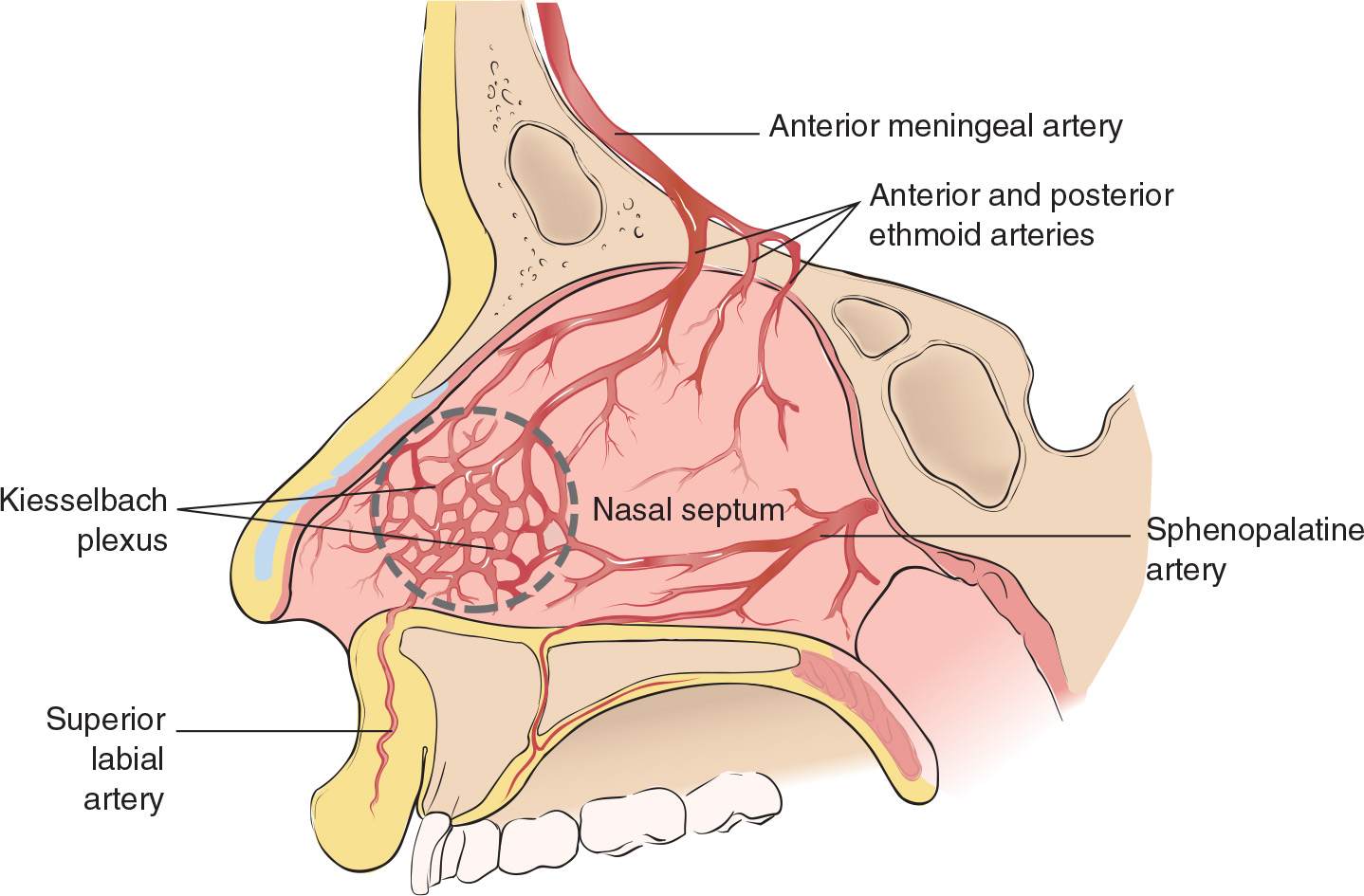
FIGURE 75.1 Anatomy of nasal septum. (From Kost SI, Post JC. Management of epistaxis. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:663, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


