![]() Pericardial tamponade with hemodynamic decompensation
Pericardial tamponade with hemodynamic decompensation
![]() Pulseless electrical activity with clinical suspicion of tamponade or with ultrasonographic evidence of pericardial effusion
Pulseless electrical activity with clinical suspicion of tamponade or with ultrasonographic evidence of pericardial effusion
CONTRAINDICATIONS
![]() None for the unstable patient
None for the unstable patient
![]() Coagulopathy is a relative contraindication
Coagulopathy is a relative contraindication
RISKS/CONSENT
![]() In the emergent situation no consent is required. Consent is implied.
In the emergent situation no consent is required. Consent is implied.
![]() For risks, see “Complications” section below
For risks, see “Complications” section below
LANDMARKS
![]() Anatomic Approaches
Anatomic Approaches
![]() Subxiphoid
Subxiphoid
![]() Needle is inserted between the xiphoid process and the left costal margin in a 30- to 45-degree angle to the skin
Needle is inserted between the xiphoid process and the left costal margin in a 30- to 45-degree angle to the skin
![]() Recommendations regarding needle aim vary widely, including right shoulder, sternal notch, and left shoulder
Recommendations regarding needle aim vary widely, including right shoulder, sternal notch, and left shoulder
![]() Parasternal approach (more common with bedside ultrasonography)
Parasternal approach (more common with bedside ultrasonography)
![]() Needle is inserted perpendicular to the skin in the left fifth intercostal space immediately lateral to the sternum
Needle is inserted perpendicular to the skin in the left fifth intercostal space immediately lateral to the sternum
![]() Ultrasound-guided approach
Ultrasound-guided approach
![]() Place a 3.5- to 5.0-MHz probe in the subcostal position to directly visualize both the area of maximal effusion and location of vital structures
Place a 3.5- to 5.0-MHz probe in the subcostal position to directly visualize both the area of maximal effusion and location of vital structures
![]() Insert needle in the left chest wall using a parasternal approach where the largest pocket of fluid is seen
Insert needle in the left chest wall using a parasternal approach where the largest pocket of fluid is seen
![]() General Basic Steps
General Basic Steps
![]() Semiupright position
Semiupright position
![]() Local analgesia
Local analgesia
![]() Sterilize local area
Sterilize local area
![]() Insert 18-gauge spinal needle
Insert 18-gauge spinal needle
![]() Aspirate while advancing
Aspirate while advancing
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() A 100% oxygen via face mask should be administered if patient is conscious and nonintubated. Consider transiently decreasing tidal volume by 10% to 15% for intubated patients.
A 100% oxygen via face mask should be administered if patient is conscious and nonintubated. Consider transiently decreasing tidal volume by 10% to 15% for intubated patients.
![]() Ensure continuous cardiac and pulse oximetry monitoring
Ensure continuous cardiac and pulse oximetry monitoring
![]() Patient should be placed in the semiupright position (15–30 degrees) if possible to pool pericardial fluid dependently
Patient should be placed in the semiupright position (15–30 degrees) if possible to pool pericardial fluid dependently
![]() If the patient is awake, local analgesia should be utilized
If the patient is awake, local analgesia should be utilized
![]() Sterilize locally with chlorhexidine or povidone–iodine solution, and use sterile gloves and universal precautions
Sterilize locally with chlorhexidine or povidone–iodine solution, and use sterile gloves and universal precautions
![]() Procedural Steps
Procedural Steps
![]() Attach an 18-gauge spinal needle to a 10- to 30-mL syringe
Attach an 18-gauge spinal needle to a 10- to 30-mL syringe
![]() Attach an alligator clip to the base of the needle and the other end to the precordial (V) lead of the electrocardiogram (ECG) machine to monitor for ST elevations indicating penetration of the myocardium (FIGURES 10.1–10.3)
Attach an alligator clip to the base of the needle and the other end to the precordial (V) lead of the electrocardiogram (ECG) machine to monitor for ST elevations indicating penetration of the myocardium (FIGURES 10.1–10.3)
![]() Using either a subxiphoid or parasternal approach (see “Landmarks” section above for details), insert and advance the spinal needle while gently aspirating the syringe, preferably with ultrasonographic assistance
Using either a subxiphoid or parasternal approach (see “Landmarks” section above for details), insert and advance the spinal needle while gently aspirating the syringe, preferably with ultrasonographic assistance
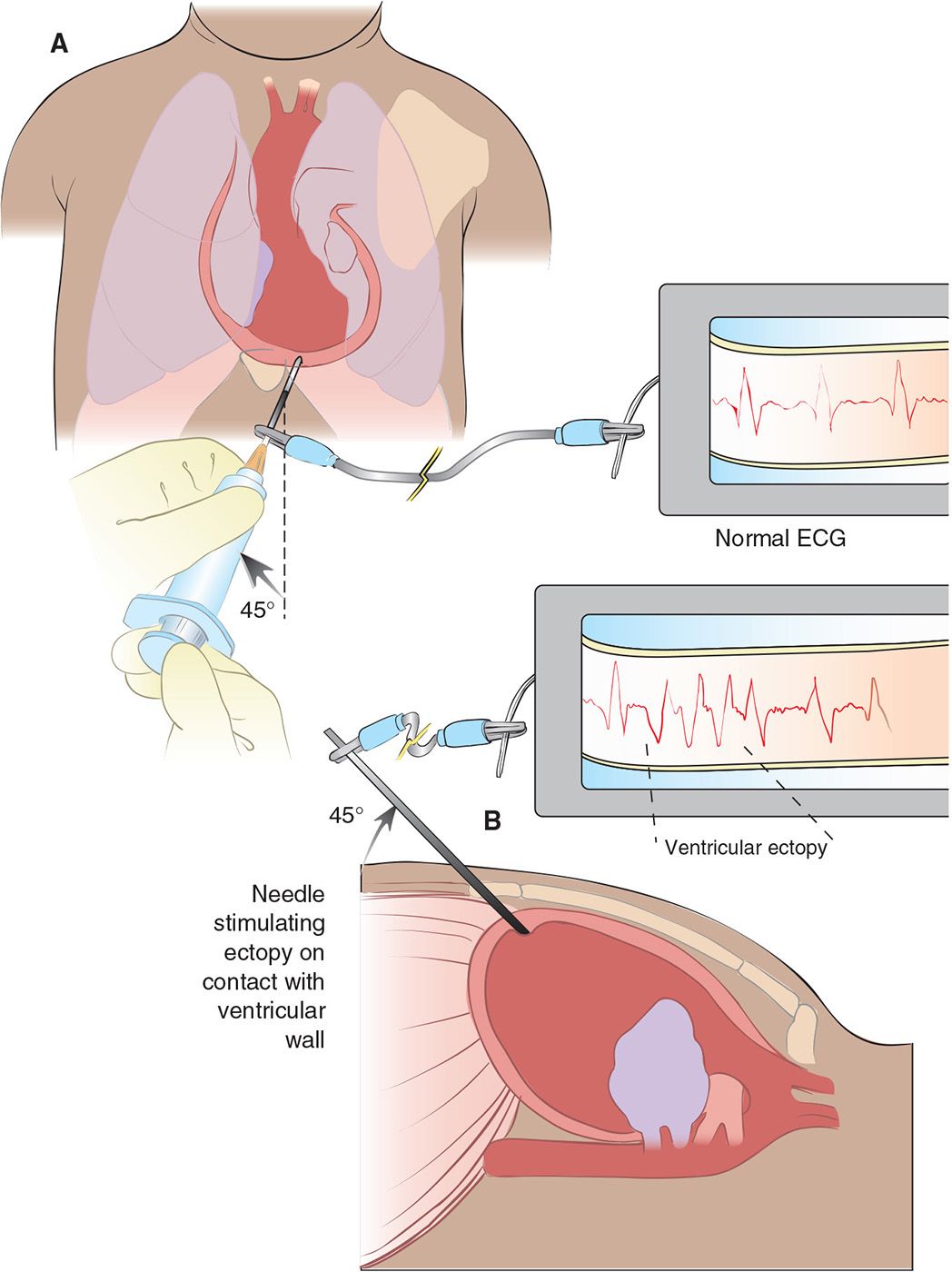
FIGURE 10.1 Attaching an ECG lead to the pericardiocentesis needle will allow you to identify when the needle contacts the ventricular wall. (From Reeves SD. Pericardiocentesis. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Philadelphia, PA: Williams & Wilkins; 1997:780, with permission.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


