15 Emergencies in the First Weeks of Life
 Key Points
Key Points• Premature infants are at higher risk for most serious neonatal illnesses.
• Congenital heart and gastrointestinal anomalies are commonly manifested during the first month of life.
• A complete set of vital signs, including weight (undressed), is required for assessment and treatment of neonatal patients.
• The majority of neonates who have experienced an apparent life-threatening event have a normal appearance at the time of arrival at the emergency department.
• Laboratory work-up of infants after an apparent life-threatening event who have normal perinatal histories and normal findings on physical examination is most often unproductive.
• An echocardiogram may help distinguish between pulmonary and cardiac causes of cyanosis.
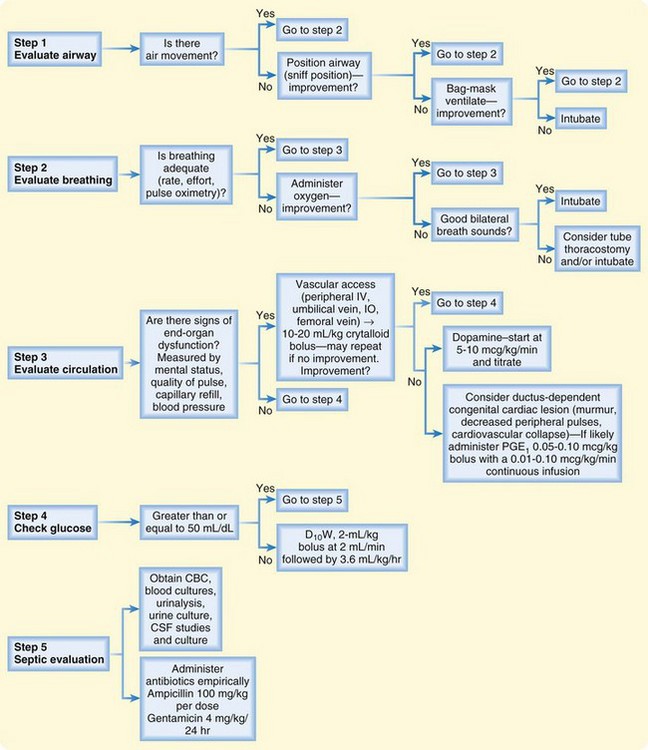
• Figure 15.1 summarizes the initial evaluation and management of seriously ill infants in the emergency department.
In 2007 the infant (child <1 year old) death rate was 686.9 per 100,000 population. This death rate is not approached again until the sixth decade of life. Two thirds of the deaths that occur in the first year of life do so in the first month.1
The Normal Neonate
Vital Signs
The core temperature in an infant is the same as that in an adult. Fever is generally recognized as a temperature higher than 38° C (100.4° F). Any temperature lower than 36.1° C (97° F) should raise concern for hypothermia. Because of limited thermoregulatory ability, neonates should be examined and treated in a warm ambient environment. See Table 15.1 for normal neonatal vital signs.
Table 15.1 Normal Vital Signs in Neonates
| Heart rate | 120-160 beats/min |
| Respiratory rate | 40-60 breaths/min |
| Blood pressure | Systolic pressure > 60 mm Hg |
| Temperature | 36.1-38° C (97-100.4° F) |
Apnea and Apparent Life-Threatening Events
Epidemiology
General estimates suggest that between 0.5% and 6.0% of infants will experience an apparent life-threatening event (ALTE). A prospective Austrian study conducted from 1993 to 2001 revealed an incidence of 2.46 per 1000 live births.2 In this study more than 60% of the events occurred in infants 2 months or younger.
Pathophysiology
ALTE is not a single disease entity but rather a constellation of signs and symptoms of numerous diseases that can have lethal consequences. The 1986 National Institutes of Health Consensus Development Conference on Infantile Apnea and Home Monitoring defined ALTE as “an episode that is frightening to the observer and is characterized by some combination of apnea (central or occasionally obstructive), change in color (usually cyanotic or pallid, but occasionally erythematous or plethoric), marked change in muscle tone (usually marked limpness), choking, or gagging.”3
The conventional definition of apnea is absence of breathing for 20 seconds or for a shorter period if associated with clinical signs such as cyanosis, hypotonia, and bradycardia. Because periods of apnea of up to 30 seconds have been observed in normal, healthy, asymptomatic term and preterm infants, the duration of apnea does not seem to be as clinically important as apnea associated with signs and symptoms.4 Apnea should be distinguished from the normal periodic breathing of newborns, which is characterized by irregular breathing and episodes of pauses. This latter pattern is more commonly seen in premature infants during sleep. Although similarities exist, ALTE is now considered a different pathophysiologic entity from sudden infant death syndrome.
Presenting Signs and Symptoms
The majority of neonates who have experienced an ALTE have a normal appearance at the time of arrival at the ED. Stratton et al. reported a prehospital study of 60 cases of ALTE in which 83% of the infants were asymptomatic by the time that emergency medical service personnel arrived.5 A comprehensive history and a thorough physical examination should be performed. One study showed that the history and physical examination were helpful in diagnosing the cause of ALTE in 70% of cases.6 The history should consist of a detailed description of the event, a prenatal and perinatal history, a review of systems, and a family history (especially child deaths, neurologic diseases, cardiac diseases, and congenital problems). Box 15.1 lists essential historical questions in these cases. A detailed physical examination should pay particular attention to the neurologic, respiratory, cardiac, and developmental components. Evidence of child abuse should be sought, including a funduscopic examination for retinal hemorrhage.
Box 15.1 Historical Questions to Ask the Caregiver of an Infant Who Has Had an Apparent Life-Threatening Event or Apnea
What was the appearance of the infant when found?
What was the infant doing when the episode occurred?
Were any interventions (cardiopulmonary resuscitation) necessary?
Was the infant awake or asleep when the event occurred?
What was the infant’s body position?
Was the infant alone in the bed?
When was the last time that the infant ate?
Was the infant sick or well in the time before the event?
Is there any history of trauma?
Is there a family history of sudden infant death syndrome or apparent life-threatening event?
* A trick that an emergency physician (EP) can use to help the caregiver answer this question is as follows: (1) the EP asks the caregiver to look at him or her, (2) the EP says “Go,” and (3) the caregiver says “Stop” when he or she thinks that the time that has passed matches the time that the event ended.
Differential Diagnosis and Medical Decision Making
ALTEs and apnea are clinical manifestations that have many causes, as summarized in Box 15.2. The most common organ systems involved (in order of decreasing frequency) are the gastrointestinal, neurologic, respiratory, cardiac, metabolic, and endocrine systems. The cause of ALTE in an individual patient is likely to be discovered only about 50% of the time.
Box 15.2 Causes of Apparent Life-Threatening Events
Diagnostic testing is best guided by the history and physical examination. Laboratory tests have been shown to be contributory to the diagnosis only 3.3% of the time if the results of the history and physical examination were noncontributory.6 An Israeli study concluded that diagnostic testing has low yield in infants with normal perinatal histories and normal findings on physical examination.7
Disposition
Historically it has been the practice that all infants with apnea or ALTE be admitted for observation. Some studies suggest that certain low-risk infant groups might be able to be discharged home from the ED.8,9 Box 15.3 lists low-risk criteria for ALTE. An infant meeting all the criteria in this box would have a very low probability of experiencing an adverse outcome. Otherwise, it is prudent to admit the infant for observation and in-patient evaluation by a pediatric specialist.
Excessive Crying and Irritability
Epidemiology
Crying peaks in infancy at 6 weeks of age with an average crying time of 3 hours per day. More of the crying time is clustered in the late afternoon and evening. Forty percent of these infants cry for 30 minutes or longer at one time, 75% of whom have the longest crying spells between 6 and 12 PM.10 The prevalence of excessive crying varies between 1.5% and 11.9%, depending on the definition of excessive crying.11
Presenting Signs and Symptoms
Box 15.4 lists important questions to ask the caregiver of an afebrile infant with excessive crying. Table 15.2 lists possible physical findings in these infants.
Box 15.4 Historical Questions to Ask the Caregiver of an Afebrile Infant with Acute and Excessive Crying
Was the crying gradual or sudden in onset?
How long has the child been crying?
Were there any potential inciting events (trauma, immunizations)?
Has the child been sick or had a fever?
Has any change in feeding pattern or stooling taken place?
Did the infant have any significant birth or perinatal problems?
Table 15.2 Potential Abnormalities in Crying Infants Found on Physical Examination
| FINDINGS AND POSSIBLE DIAGNOSES | |
|---|---|
| Inspection | |
| General | Ill appearance: |
| Sepsis, meningitis, other infectious process | |
| Dehydration | |
| Congenital heart disease (cardiogenic shock), supraventricular tachycardia | |
| Volvulus, bowel perforation, incarcerated hernia, intussusception, appendicitis | |
| Intracranial hemorrhage (traumatic/nontraumatic) | |
| Hypoglycemia, inborn error of metabolism | |
| Skin | Trauma, abscess, cellulitis |
| Eyes, ears, nose, throat | Corneal abrasion, foreign body, teething |
| Abdomen, genitourinary structures | Hernia, hair tourniquet on penis, paraphimosis |
| Extremities/clavicles | Fracture deformity (accidental/nonaccidental), digit hair tourniquet |
| Palpation | |
| Head | Trauma Fontanelle: Dehydration, increased intracranial pressure |
| Chest | Clavicular fracture |
| Abdomen | Tenderness/peritoneal signs: Volvulus, bowel perforation, appendicitis, intussusception, incarcerated hernia |
| Genitourinary structures | Testicular torsion |
| Extremities/clavicles | Trauma, fracture, soft tissue infection |
| Auscultation | |
| Heart | Decreased pulses: Congenital heart disease, septic shock |
| Lungs | Murmur: Congenital heart disease |
| Tachycardia: Supraventricular tachycardia, congestive heart failure | |
| Stridor: Upper airway obstruction | |
| Wheezing: Airway foreign body, bronchiolitis | |
| Rales: Pneumonia, congestive heart failure | |
| Abdomen | Hypoactive/hyperactive or absence of bowel sounds: Volvulus, intussusception, appendicitis, incarcerated hernia |
Differential Diagnosis and Medical Decision Making
The first differentiation that the clinician must make is whether the child is febrile (see the section “Fever”). In an afebrile infant the chronicity of the crying is important. Is the crying an acute single episode, or has it been an ongoing problem for some time?
The latter describes colic, which affects a large subgroup of excessively crying infants. Classically, colic has been described by the rule of threes—crying for 3 hours per day, for at least 3 days per week, for 3 weeks. Scores of theories concerning the etiology of colic have been proposed; such theories range from physiologic disturbances (cow’s milk allergies, gastrointestinal reflux, hypocontractile gallbladder, and other gastrointestinal disturbances), to infant temperament and maternal response, to deficiencies in parenting practices.12 No single cause has been identified.
No pharmacologic agent has been listed as being both safe and efficacious for the treatment of colic. Anticholinergic agents have been found to be more effective than placebo but are associated with apnea and should not be administered to infants younger than 6 months.13 Many other interventions have been proposed for colic, such as having the infant in a car, specific ways to hold the infant, use of white noise, crib vibrators, and herbal teas. None have been shown to be particularly beneficial, however. The EP should reassure parents that there is no ideal treatment of colic, that their child is normal, that the infant will outgrow the colic, and that colic has no long-term sequelae.
A retrospective study involving 237 afebrile children younger than 1 year brought to the ED with the chief complaint of crying or fussiness revealed that 5.1% had a serious underlying etiology. The final diagnosis in the 237 patients was made by the history and physical examination alone in 66% of cases. Only 0.8% of the diagnoses were made by diagnostic evaluation alone. These authors concluded that afebrile crying infants younger than 1 month should undergo urinalysis.14
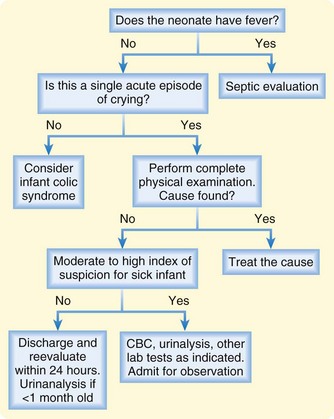
A suggested approach to the ED evaluation of an excessively crying child is presented in Figure 15.2.
Cyanosis
Differential Diagnosis and Medical Decision Making
An easy method of classifying cyanosis is by causative organ system (Box 15.5). The cardiac and respiratory systems are responsible for the large majority of cases of neonatal cyanosis. Distinguishing between these two categories can be difficult but is necessary for optimal management of the patient.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


