Chapter 16 Electrosurgery
HISTORICAL BACKGROUND
In the 1800s researchers around the world were independently conducting experiments with electricity. In both England and America Michael Faraday (1791–1867) and Joseph Henry (1797–1878) were conducting experiments on the relationship between magnetism and electricity. They discovered that a moving magnet could induce an electrical current in a conductive wire. Electromagnetism was a very important principle that led to improved electromedical devices (Goldwyn, 1979).
The research conducted in the years between 1881 and 1900 saw electrical current moved into the higher-frequency ranges. In 1881 William J. Morton reported that current in the 100-kHz range did not produce the painful tissue effects of current in the lower-frequency ranges. By 1891 Arsenne d’Arsonval of France had documented that the alternating current frequency could safely be lowered to 100 kHz (Pearce, 1986).
An early use of electrosurgery clinically was by Joseph A. Riviere. While treating a musician with electricity for insomnia, Riviere accidentally touched one of the wires on a device he was using and produced a spark. This incident prompted Riviere to use the spark on an ulcer on the musician’s hand. Repeated treatments resulted in healing of the ulcer. Riviere reported his results at the First International Congress of Medical Electrology and Radiology in Paris in 1900. This is said to be the first surgical use of high-frequency current to treat a human condition (Kelly and Ward, 1932).
The advances Cushing made in surgical care and specifically neurosurgery are legendary. He was one of the first proponents of blood pressure monitoring during surgery and used primarily local anesthesia. There were also great advances made in controlling blood loss during surgery through the methods that Cushing used. There were, however, still patients that were considered inoperable due to the concern of uncontrolled bleeding. Cushing’s first true consideration of the use of electrosurgery seems to have occurred at a medical conference in the summer of 1925. Samuel Harvey and John Morton, both residents of Cushing’s, were watching an electrosurgery demonstration when Cushing joined them. One of them jokingly suggested that Cushing use the machine on the brain. Instead of discounting the possibility, Cushing stopped and looked thoughtfully at the demonstration (Voorhees et al, 2005). Cushing later visited Bovie’s laboratory at Harvard to inquire further about his electrical machine.
ELECTROSURGERY
Basic Principles of Electricity
1. Electricity always follows the path of least resistance.
2. Electricity always seeks to return to ground (Columbia Encyclopedia, 2001).
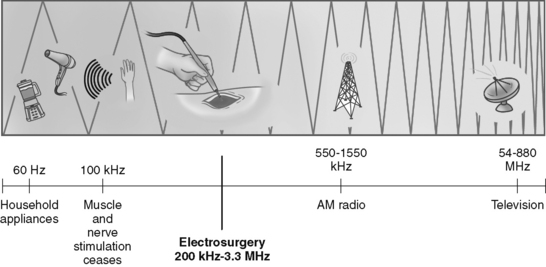
AC changes, or alternates, direction of the electrical flow. The frequency of these alterations is measured in cycles per second or Hertz (Hz), with 1 Hz being equal to one cycle per second. Household current alternates at 60 cycles per second, as does much of the electrical equipment used in operating rooms. Alternating current at 60 Hz can cause tissue injury. As early researchers discovered, neuromuscular stimulation ceases at about 100,000 Hz as the alternating current moves into the radio-frequency range. Electrosurgery generators take 60-cycle household current and raise it to the radio-frequency range of 200,000 Hz to 3.3 MHz (Figure 16-1). As electrons flow through a conductor, that flow is measured in amperes, or amps (Hutchisson et al, 1998).
Electrosurgery Waveforms
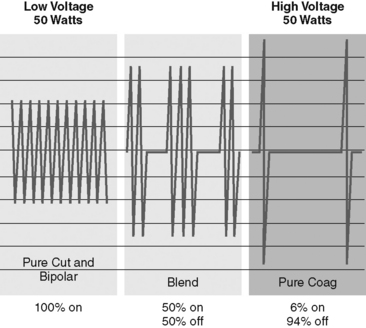
One of the important discoveries during the early development of the electrosurgery generator was that the electrical output from the generators could be manipulated to produce different waveforms, or electrosurgical modes. There are three basic waveforms that have distinct tissue effects. The modes or waveforms are cut, fulguration, and blend (Figure 16-2).
Related posts:
 Preventing Surgical Site Infections
Safety in the Perioperative Setting: Vendor Support
Preventing Surgical Site Infections
Safety in the Perioperative Setting: Vendor Support
 To Count or Not to Count: A Surgical Misadventure
To Count or Not to Count: A Surgical Misadventure
 Laser Risks and Preventive Measures for the Staff
Laser Risks and Preventive Measures for the Staff
 Incidence of Deep Venous Thrombosis in the Surgical Patient Population and Prophylactic Measures to Reduce Occurrence
Incidence of Deep Venous Thrombosis in the Surgical Patient Population and Prophylactic Measures to Reduce Occurrence
 Fire Prevention in the Perioperative Setting: Perioperative Fires Can Occur Everywhere
Fire Prevention in the Perioperative Setting: Perioperative Fires Can Occur Everywhere
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


